Chapter: Obstetrics and Gynecology: Endometriosis
Diagnosis of Endometriosis
DIAGNOSIS
Endometriosis should be suspected
in patients with the pre-viously described symptoms. Many symptomatic women
have normal findings on pelvic examination. The
diagnosis ofendometriosis can be substantiated only by direct visualization
during laparoscopy or laparotomy confirmed by tissue biopsy. Thepresence of
two or more of the following histologic fea-tures is used as the threshold
criteria for the diagnosis by a pathologist:
· Endometrial
epithelium
· Endometrial
glands
· Endometrial
stroma
· Hemosiderin-laden
macrophages
Because tissue confirmation of
the diagnosis of endo-metriosis requires a surgical procedure, investigators
have searched for a noninvasive alternative. Increased serum CA-125 levels have
been correlated with moderate to severe endometriosis. However, because CA-125
levels may be elevated in many conditions, the clinical utility of using it as
a diagnostic marker is limited.
Imaging studies, such as
ultrasonography, magnetic resonance imaging, and computed tomography appear to
be useful only in the presence of a pelvic or adnexal mass. Ultrasonography may
be used to visualize ovarian endo-metriomas, which typically appear as cysts
containing low-level, homogeneous internal echoes consistent with old blood.
Magnetic resonance imaging may detect deeply infiltrating endometriosis that
involves the uterosacral lig-aments and the cul-de-sac, but lacks sensitivity
in detecting rectal involvement.
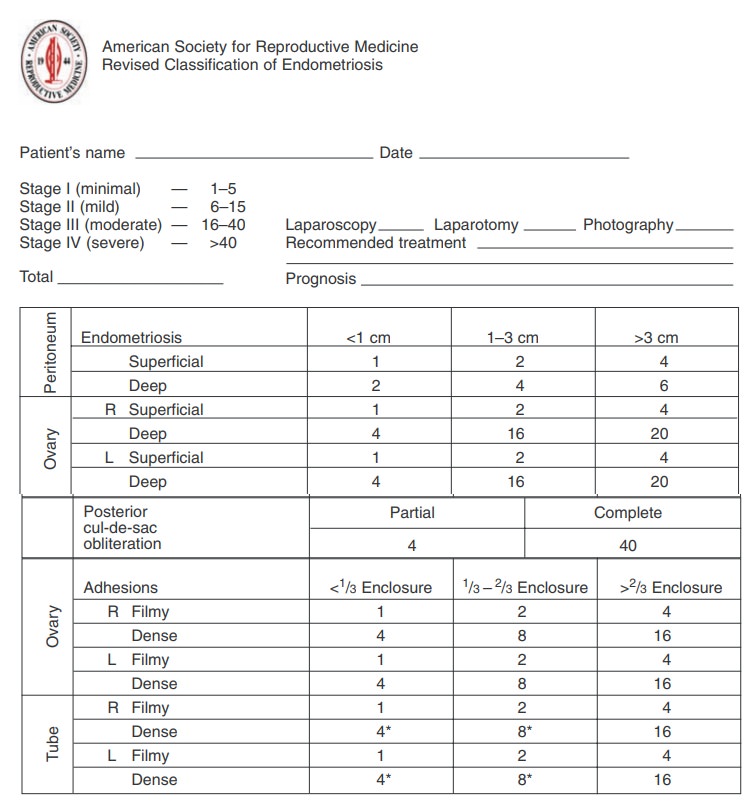
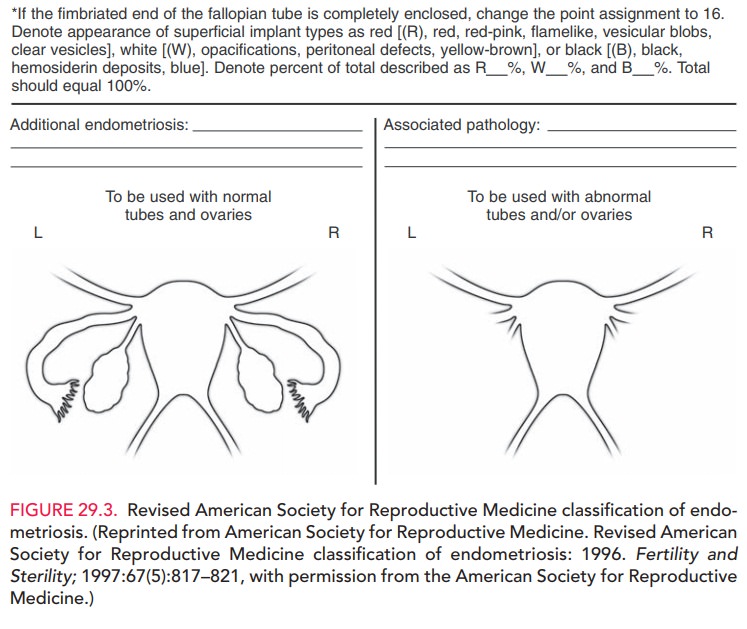
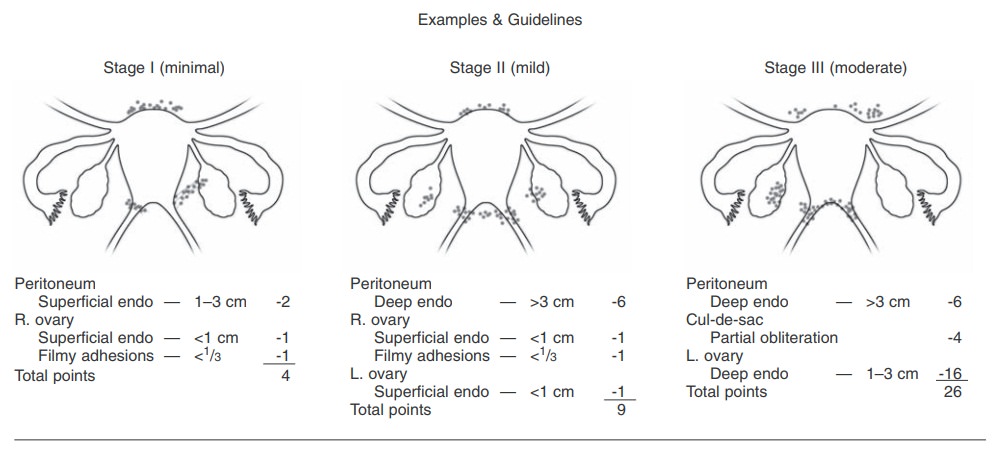
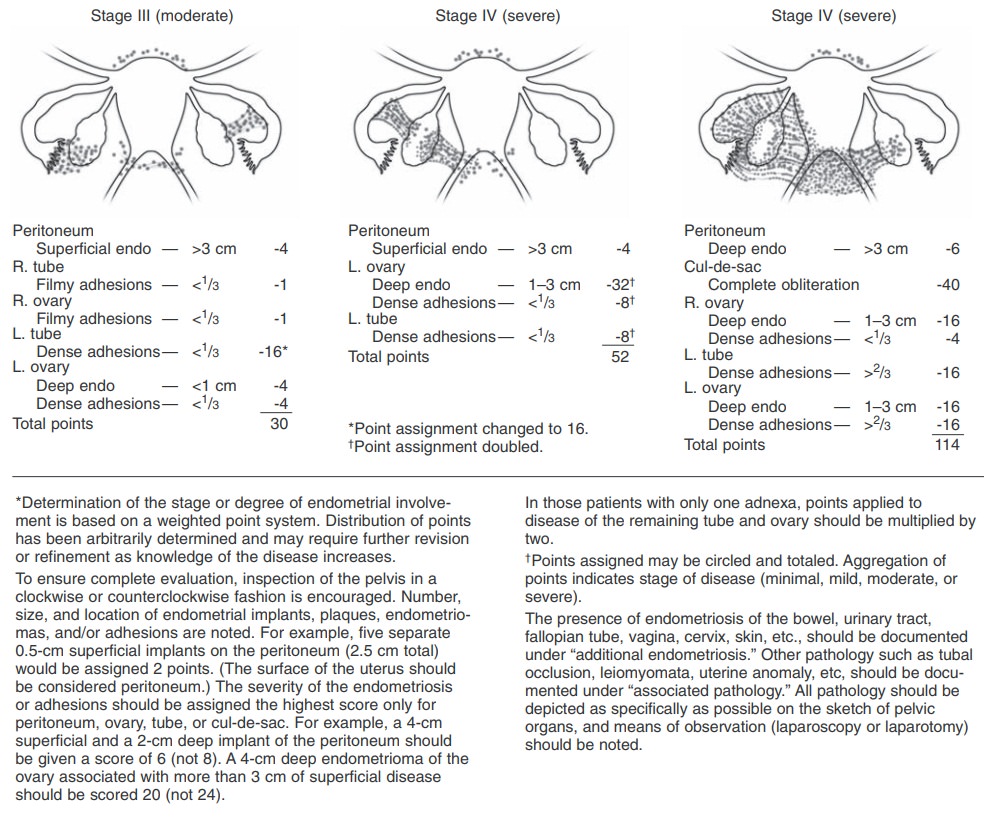
Once endometriosis is diagnosed,
its extent and sever-ity should be documented. The most widely accepted
clas-sification system has been established by the American Society for
Reproductive Medicine (Fig. 29.3). While this classification scheme has
limitations, it provides a uniform system for recording findings and comparing
the results of various therapies.
Related Topics