Chapter: Pathology: Respiratory Pathology
Pulmonary Neoplasia
PULMONARY NEOPLASIA
Lung
cancer is the leading cause of cancer death among both men and
women; it hasbeen increasing in women (increased smoking) in the past few
decades. It occurs most commonly age 50–80. Major risk factors include
cigarette smoking, occu-pational exposure (asbestosis, uranium mining,
radiation, etc.), passive smoking, and air pollution. Clinical features include
cough, sputum production, weight loss, anorexia, fatigue, dyspnea, hemoptysis,
and chest pain. Obstruction may produce focal emphysema, atelectasis,
bronchiectasis, or pneumonia.
Common
genetic mutations in lung cancer involve the oncogenes MYCL (small cell carcinomas) and KRAS (adenocarcinomas); tumor suppressor genes: TP53 and RB1.
Adenocarcinoma
is more commonly seen in women and nonsmokers. Grossly,
itcauses a peripheral gray-white mass, and the tumor may develop in areas of
paren-chymal scarring (scar carcinoma). Microscopically, common patterns
include acinar, papillary, mucinous, and solid. The precursor lesion—atypical
adenomatous hyper-plasia—progresses to adenocarcinoma in situ (noninvasive
well- differentiated tumor <3 cm) and to minimally invasive tumor (invasion
no more than 5 mm) before progressing to invasive adenocarcinoma.
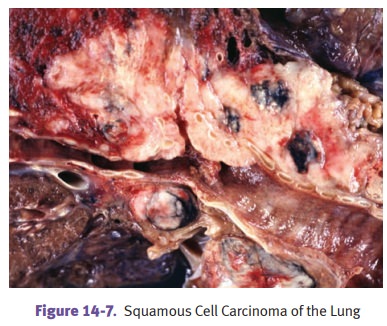
Squamous
cell carcinoma (SCC) is strongly related to smoking and
affects malesmore than females. Squamous cell carcinoma arises from bronchial
epithelium after a progression:
metaplasia
→ dysplasia → carcinoma in situ →
invasive carcinoma
Pathologically,
the tumor grossly causes a gray-white bronchial mass, usually cen-trally
located. Microscopically, well-differentiated tumors show invasive nests of
squamous cells with intercellular bridges (desmosomes) and keratin production
(“squamous pearls”).
Small
cell carcinoma has a strong association with smoking, and affects males
morethan females. This neuroendocrine tumor is very aggressive, with rapid
growth and early dissemination. Small cell carcinoma is commonly associated
with paraneo-plastic syndromes.
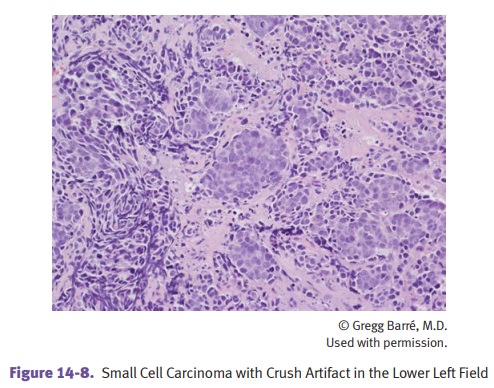
Pathologically,
gross examination demonstrates central, gray-white masses. Micro-scopic
examination shows small round or polygonal cells in clusters, and electron
microscopy shows cytoplasmic dense-core neurosecretory granules.
Large
cell carcinoma has large anaplastic cells without
evidence of differentiation.
Intrathoracic
spread of lung cancer is to lymph nodes, particularly hilar,
bronchial,tracheal, and mediastinal;
pleura (adenocarcinoma); and lung apex causing Horner syndrome (Pancoast tumor).
·
Obstruction of the superior vena
cava by tumor causes superior vena
cavasyndrome, characterized by distended head and neck veins, plethora,
andfacial and upper arm edema.
·
Esophageal
obstruction can cause dysphagia.
·
Recurrent laryngeal nerve involvement causes hoarseness,
while phrenic nerve damage causes diaphragmatic paralysis.
Extrathoracic sites of
metastasis include adrenal (>50%), liver, brain, and bone.
Paraneoplastic syndromes
·
Endocrine/metabolic syndromes include
Cushing syndrome secondary to ACTH production, SIADH secondary to ADH
production, and hypercalcemia secondary to PTH production (squamous cell
carcinoma).
·
Eaton-Lambert syndrome
·
Acanthosis nigricans
·
Hypertrophic pulmonary
osteoarthropathy is characterized by periosteal new bone formation with
clubbing and arthritis.
Treatment
of non–small cell lung cancer is with surgery, and treatment of small cell lung
cancer is with chemotherapy and radiation. Despite treatment, the prognosis is
poor, with overall 5-year survival 16%.
Bronchial
carcinoids occur in a younger age group (mean age 40 years) and
typi-cally produce a polypoid intrabronchial mass or plaque; it is
characterized on light microscopy by small, round, uniform cells growing in
nests (organoid pattern), and on electron microscopy by cytoplasmic dense-core
neurosecretory granules. Atypi-cal carcinoid is more aggressive than typical
carcinoid.
Metastatic
carcinoma is the most common malignant neoplasm in the lung. It
typi-cally causes multiple, bilateral, scattered nodules; common primary sites
include breast, stomach, pancreas, and colon.
Hamartomas
are benign tumors; they occur more commonly in middle-aged
adultsbut also occur in children. They can appear as coin lesions on chest
x-ray. Micro-scopically, they are comprised of nonencapsulated fibromyxoid
tissue. Carney triad is the finding of a hamartoma with a predominantly
cartilaginous component (pul-monary chondroma), an extra-adrenal paraganglioma
and a gastric gastrointestinal stromal tumor.
Related Topics