Chapter: Essentials of Psychiatry: Psychopathology Across the Life-Cycle
Problems of Childhood
Problems of Childhood
Individual Differences
Children differ from each other in ways that affect
their psy-chological functioning from birth. They differ in intelligence, in temperament
and in genetic endowment for both risk for and resilience against mental
disorder.
Intelligence is the ability to reason, plan, think
abstractly, solve problems, understand and learn. Average intelligence is
as-sociated with a score of 100 (IQ) on a standardized intelligence test. About
67% of children have IQs between 85 and 115 and about 95% between 70 and 130.
Estimates of the heritability of IQ range from 0.4 to 0.8 (Plomin, 1990)
indicate that heredity plays a larger role than environment. Higher
intelligence is correlated with successful adaptation in life, and
substantially reduced in-telligence is associated with developmental and
behavioral prob-lems and functional impairment (see the discussion of mental
retardation).
Types of Problems
Psychopathology in childhood falls into four major
groups of problems (Table 8.2). Many of the disorders of childhood appear to be
severe forms of problems that are more or less continuously distributed, common
and “normal” occurrences. Thus, clinical depression may appear to be a severe
form of sadness and disap-pointment, conduct disorder a severe form of
aggressiveness, and anorexia nervosa a severe form of adolescent dieting and
dissat-isfaction with body shape (Rutter and Sandberg, 1985).
Estimates are that 5 to 15% of 9- to 10-year-old
children suffer from an emotional or behavior disorder of sufficient severity
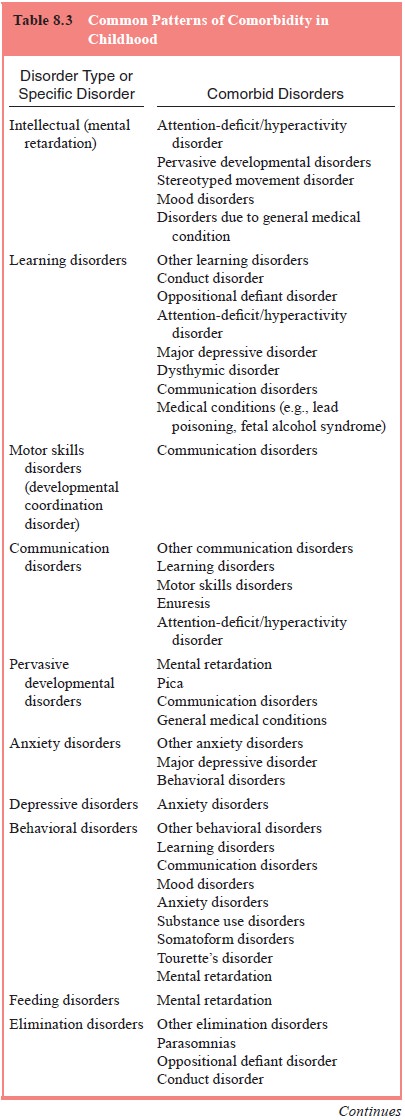
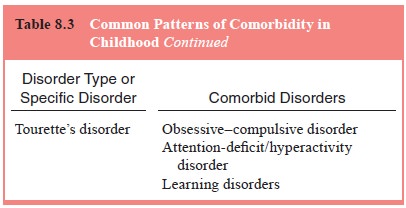
to cause impairment in everyday functioning (Cox, 1994). The co-occurrence of
several disorders (i.e., comorbidity) is common in childhood (Caron and Rutter,
1991). As can be seen in Table 8.3, comorbidity both within and between
disorder types can be observed.
Developmental Problems
Childhood is a time of growth, physical and social maturation, and the acquisition of skills necessary to deal independently and successfully with the environment. Children who are greatly delayed in their development or who never acquire the requisite skills or maturity associated with their developmental stage have developmental problems. Developmental disorders fall into five main types: intellectual, learning, motor skills, communication and pervasive developmental disorders.
The most severe developmental problems are evident
in infancy. For example, the infant with autism may manifest limited eye
contact, facial responsiveness and smiling, and may be difficult to hug or may
appear to dislike physical contact. Restricted social relationships emerge,
however, after the third or fourth year of life. For children with other
pervasive developmental disorders, infancy may be normal, with the onset of the
abnormal behavior occurring months or even years after birth. In milder forms,
such as Asperger’s syndrome (Tantum, 1988), in which communication skills are
spared, a pervasive developmental disorder may not be recognized until
preschool or the actual beginning of school. The course after diagnosis is
variable, depending on the subtype.
Emotional Problems
The emotional problems of children involve anxiety
and depression. Although these problems have counterparts in adults, children
frequently experience and express their disturbances of feelings or emotions
differently from adults. Because of their more limited vocabulary and
understanding of emotional life, children may not express their emotional
distress verbally as well as some adults do. Thus, even in the emotional
disorders of childhood, disturbances in behavior and in physical functioning
are apt to be prominent in the clinical presentation. Children are not unlike
so-called alexithymic adults, whose expression of emotions is indirect and
nonverbal.
Some children may be excessive worriers in general.
They may worry about school performance, athletic prowess, appearance and
popularity, parental expectations, potential catastrophic events, and so on.
Children who worry exces-sively are said to have generalized anxiety disorder.
Moody periods are common in children, but children may also ex-hibit prolonged
and persistent disturbances of mood, usually depression.
The manifestations of mania in younger children may
involve irritability, emotional lability, or admixtures of dys-phoria and
hypomania, as well as more typical symptoms of hyperactivity, grandiosity,
pressure of speech and distractibility (Carlson, 1990; Strober et al., 1989). As many as one-third of
children with major depressive episodes may show bipolar disorder by
adolescence (Geller et al., 1994).
Early-onset bi-polar disorders may have a poorer prognosis than later onset
disorders. Childhood major depressive disorder also appears to increase the
risk for the development of personality disorders in young adulthood (Kasen et al., 2001).
Behavior Problems
Behavior problems in children fall into the general
groupings of oppositional behavior, hyperactivity, excessive aggressiveness and
conduct disturbance. An appropriate degree of control over behavior is a
necessary development for a child to function in a family, in school, and with
peers.
Disturbances in Physical Functioning
A number of developmental tasks of childhood
involve primarily physical functions. These include developing proper eating
and sleeping habits (Wolke, 1994), bowel (Hersov, 1994) and bladder (Shaffer,
1994) control and sexual identity (Paikoff and Brooks-Gunn, 1994). Disturbances
may occur in these functions during childhood.
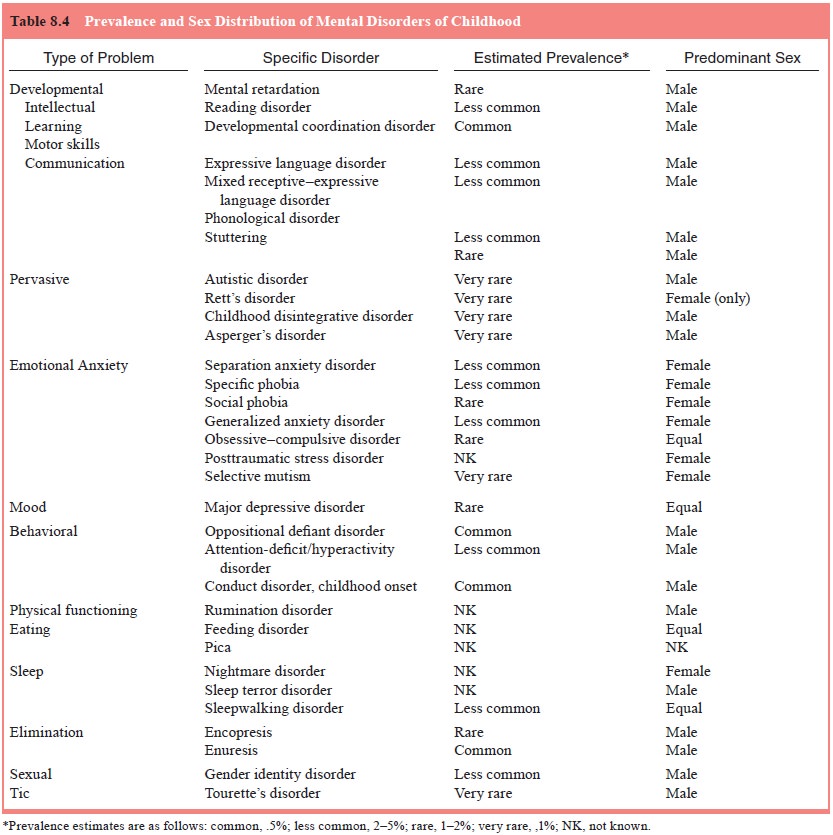
Table 8.4 summarizes the estimated prevalence and
sex distribution of DSM-IV-TR mental disorders seen in children.
Related Topics