Chapter: Clinical Anesthesiology: Anesthetic Management: Preoperative Assessment, Premedication, & Perioperative Documentation
Preoperative Evaluation
PREOPERATIVE EVALUATION
The cornerstones of an effective
preoperative evaluation are the medical history and physical examination, which
should include a complete account of all medications taken by the patient in
the recent past, all pertinent drug and contact aller-gies, and responses and
reactions to previous anes-thetics. Additionally, this evaluation should
include any indicated diagnostic tests, imaging procedures, or consultations
from other physicians. The pre-operative evaluation guides the anesthetic plan:
inadequate preoperative planning and incomplete patient preparation are
commonly associated with anesthetic complications.
The preoperative evaluation serves
multiple purposes. One purpose is to identify those few patients whose outcomes
likely will be improved by implementation of a specific medical treatment
(which in rare circumstances may require that the planned surgery be
rescheduled). For example, a 60-year-old patient scheduled for elective total
hip arthroplasty who also has unstable angina from left main coronary artery
disease would more likely survive if coronary artery bypass grafting is
performed before the elective procedure. Another purpose is to identify
patients whose condition is so poor that the proposed surgery might only
has-ten death without improving the quality of life. For example, a patient
with severe chronic lung disease, end-stage kidney failure, liver failure, and
heart failure likely would not survive to derive benefit from an 8-hour,
complex, multilevel spinal fusion with instrumentation.
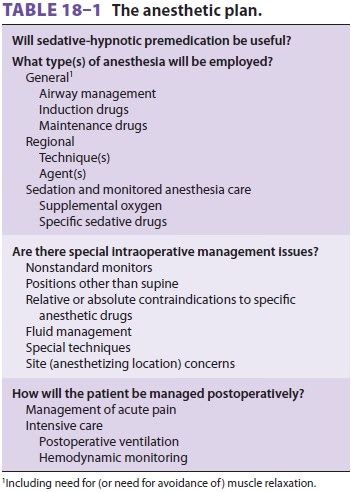
The preoperative evaluation can identify
patients with specific characteristics that likely will influence the proposed
anesthetic plan (Table 18–1). For example, the anesthetic plan may need to be
reassessed for a patient whose trachea appears diffi-cult to intubate, one with
a family history of malig-nant hyperthermia, or one with an infection near
where a proposed regional anesthetic would be
administered. Another purpose of the
evaluation is to provide the patient with an estimate of anestheticrisk.
However, the anesthesiologist should not be expected to provide the
risk-versus-benefitdiscussion for the proposed procedure; this is the
responsibility and purview of the responsible sur-geon or “proceduralist.” For
example, a discussion of the risks and benefits of robotic prostatectomy
ver-sus radiation therapy versus “watchful waiting” requires knowledge of both
the medical literature and the morbidity–mortality statistics of an individ-ual
surgeon, and it would be most unusual for an anesthesiologist to have access to
the necessary data for this discussion. Finally, the preoperative evalua-tion
is an opportunity for the anesthesiologist to describe the proposed anesthetic
plan in the context of the overall surgical and postoperative plan, pro-vide
the patient with psychological support, and obtain informed consent for the
proposed anesthetic plan from the surgical patient.
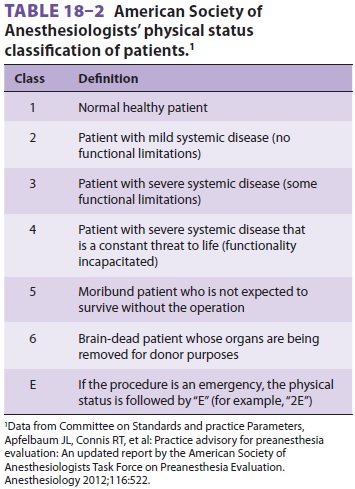
By convention, physicians in many
coun-tries use the American Society of Anesthesiologists’ (ASA) classification
to define relative risk prior to conscious sedation and surgical anesthesia (Table 18–2).
The ASA physical status classification has many advantages over all other risk
classification tools: it is time honored, simple, reproducible, and, most
importantly, it has been shown to be strongly associated with perioperative
risk. But, many other risk assessment tools are available.
Related Topics