Chapter: Modern Pharmacology with Clinical Applications: Drugs Used in Gastrointestinal Disorders
Pharmacological Modulation of Diarrhea
PHARMACOLOGICAL
MODULATION OF DIARRHEA AND CONSTIPATION BY MECHANISMS THAT DO NOT DIRECTLY
AFFECT MOTILITY
Drugs Useful for Treating Diarrhea: Adsorbents and Bulking Agents
Kaolin powder and other
hydrated aluminum silicate clays, often combined with pectin (a complex
carbohy-drate), are the most widely used adsorbent powders (e.g., Kaopectate). Kaolin is a naturally
occurring hy-drated aluminum silicate that is prepared for medicinal use as a
very finely divided powder. The rationale be-hind its use in acute nonspecific
diarrhea stems from its ability to adsorb some of the bacterial toxins that
often cause the condition. It is almost harmless and is effec-tive in many
cases of diarrhea if taken in large enough doses (2–10 g initially, followed by
the same amount af-ter every bowel movement). The adsorbents are gener-ally
safe, but they may interfere with the absorption of some drugs from the GI
tract.
Bismuth subsalicylate (Pepto-Bismol) also binds in-testinal
toxins and may coat irritated mucosal surfaces. This compound is a salicylate
and may therefore pro-duce signs of salicylate toxicity (e.g., ringing of the
ears) if taken chronically, especially with aspirin. Bismuth is radiopaque and
may interfere with radiological exami-nations. Its use may cause temporary
gray-black discol-oration of the stool and brown pigmentation of the tongue.
High dose Pepto-Bismol (8 tablets/day) has been efficacious in some patients
with diarrhea second-ary to collagenous or lymphocytic colitis.
Hydrophilic substances such
as calcium polycarbophil (FiberCon,
Equalactin), methylcellulose (Citrucel),
and various psyllium seed derivatives (Metamucil)
are natural or synthetic fiber supplements that bind water and bile salts and
may be useful in controlling diarrhea associated with the passing of
excessively watery stools.
Drugs Useful for Treating Constipation
There is a great deal of
variability in bowel habits from person to person; a normal stool frequency may
vary from three stools per week up to three stools per day. Constipation is
defined as the infrequent passage of stool. It may be secondary to sluggish
colonic motility, in which soft stool is seen throughout the colon, or to
dif-ficulties with evacuation in which firm stool is seen pri-marily in the
sigmoid and rectum.
The dangers of excessive
purging are salt and fluid loss and gradually increasing desensitization of the
bowel to normal stimuli; the latter effect forces the cathartic user to employ
larger and larger doses.
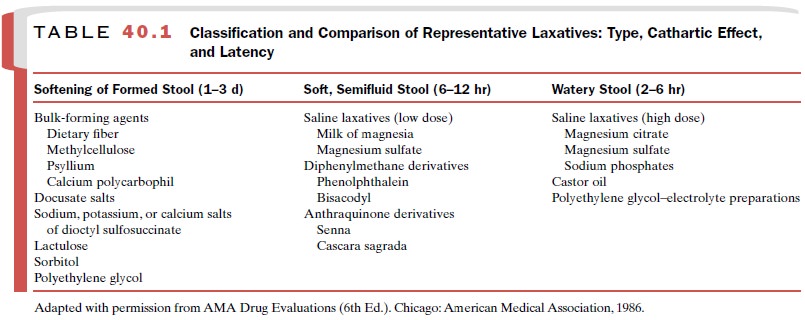
Laxatives are used to
increase stool frequency and reduce stool viscosity. Even with long-term use,
bulk laxatives and pure osmolar laxatives do not predispose patients to
formation of a cathartic-type colon and should be the initial agents used for
chronic constipa-tion after a structural obstructing lesion has been ex-cluded.
Laxatives are also used before radiological, en-doscopic, and abdominal
surgical procedures; such preparations quickly empty the colon of fecal material.
Nonabsorbable hyperosmolar solutions or saline laxa-tives are used for this
purpose. Classification and com-parison of representative laxatives are
provided in Table 40.1.
Stool Softeners
Fecal softeners are
substances that are not absorbed from the alimentary canal and act by
increasing the bulk of the feces and softening the stool so that it is eas-ier
to pass. Mineral oil has been in use for many years, either as the oil or as a
white emulsion; it is a mixture of liquid hydrocarbons. Its use has been criticized
for many reasons. It dissolves the fat-soluble vitamins and prevents their
absorption. It is itself absorbed slightly and appears in the mesenteric lymph
nodes, and if it is inhaled into the lungs (which it may be in elderly or
de-bilitated patients), it may produce inflammatory re-sponses such as lipoid
pneumonia. Its continual use, therefore, is contraindicated, although its
occasional ad-ministration in otherwise well patients is not harmful. It is
employed primarily in patients who must avoid straining at stool, including
persons with hemorrhoids and other painful anal lesions. Leakage of mineral oil
past the anal sphincter may lead to soiling of clothing.
Docusate dioctyl sodium
sulfosuccinate (Colace), dioctyl
calcium sulfosuccinate (Surfak), and
dioctyl potassium sulfosuccinate (Diocto-K)
are surface-active agents that produce fecal softening in 1 or 2 days. By means
of its detergent properties, docusate allows water to penetrate and soften
colonic contents when it is ad-ministered as a retention enema. Orally ingested
do-cusate may also act as a stool softener by stimulating the secretion of
water and electrolytes into the intes-tinal lumen. Docusate has been used both
alone and in combination with other laxatives. Although by itself it appears to
be relatively nontoxic, it may, when taken in combination with other laxatives,
increase their absorp-tion and lead to liver toxicity. Caution is necessary
when docusate is prescribed together with mineral oil, since the detergent
increases the absorption of the oil.
Bulk Forming Laxatives
The bulk-forming laxative group includes the hy-drophilic substances described previously: calcium polycarbophil (FiberCon, Equalactin), methylcellulose (Citrucel), and various psyllium seed derivatives (Metamucil). All act by increasing the bulk of the feces, part of this action being due to their capacity to attract water and form a hydrogel. The increased volume of fe-ces stretches the walls of the GI tract and stimulates peristalsis. Their action may not be evident for 2 to 3 days after starting treatment. Because their use results in increased water content in the feces, the patient should be advised to drink adequate amounts of water; otherwise dehydration may result.
The use of high-fiber diets has recently received a
great deal of publicity, and many claims have been made for the value of such
diets. Fiber in the diet is de-rived entirely from plant material, either from
fruit and vegetables or from cereals, the latter being known as bran. The fiber content in each case is
a complex carbo-hydrate in the form of cellulose, pectin, and lignin. These
fibers pass through the human GI tract relatively unaltered by enzymes.
A high-fiber diet is
effective in the prevention of constipation and diverticulitis. Claims also
have been made that such diets prevent cancer of the colon. Such allegations
require further study.
Since clear advantages accrue
from a high-bran diet (a reduction in both constipation and diverticulitis) and
since there is no associated toxicity, a
bulk-forming lax-ative is the laxative of choice for constipated patients.
Osmotic Laxatives
Osmotic laxatives (e.g.,
lactulose, sorbitol) are poorly absorbed or nonabsorbable compounds that draw
addi-tional fluid into the GI tract. Lumen osmolality in-creases, and fluid
movement occurs secondary to os-motic pressure. Lactulose is a synthetic
disaccharide that is poorly absorbed from the GI tract, since no mammalian
enzyme is capable of hydrolyzing it to its monosaccharide components. It
therefore reaches the colon unchanged and is metabolized by colonic bacteria to
lactic acid and to small quantities of formic and acetic acids. Since lactulose
does contain galactose, it is con-traindicated in patients who require a
galactose-free diet. Metabolism of lactulose by intestinal bacteria may result
in increased formation of intraluminal gas and abdominal distention. Lactulose
is also used in the treatment of hepatic encephalopathy.
Polyethylene glycol (Miralax) is another osmotic laxative
that is colorless and tasteless once it is mixed.
Saline Laxatives
Saline laxatives are soluble
inorganic salts that contain multivalent cations or anions (milk of magnesia,
mag-nesium citrate, and sodium phosphate [Fleet
Phospho Soda]). These charged
particles do not readily cross the intestinal
mucosa and therefore tend to remain in the lumen of the GI tract, where they
help retain fluid through the osmotic effect exerted by the unabsorbed ions.
The volume in the GI tract is increased, distending the colon and producing a
physiological stimulus for peristalsis through activation of stretch receptors.
This explanation of the mechanism by which the saline laxa-tives exert their
effects, however, may be too simplistic, since active secretion of fluid into
the gut lumen has been documented following the administration of
mag-nesium-containing agents.
These salts should always be
given with substantial amounts of water; otherwise the patient may be purged at
the expense of body water, resulting in dehydration. Sodium-containing
laxatives should not be used in pa-tients with congestive heart failure, since
the patient may absorb excessive sodium. Similarly, in cases of renal failure,
magnesium or phosphate-containing products should not be used, since the loss
of a renal clearance of these ions may result in cumulative toxic levels
despite their minimal absorption.
Enemas may contain water, salts, soap, mineral de-tergent (docusate
potassium), or hypertonic (sorbitol, sodium phosphate–biphosphate) fluids.
These are con-venient and generally safe for short-term use. Many of these
solutions irritate the mucosa and may produce ex-cessive mucus in the stool.
Excessive use of these enema products may result in water intoxication and
hypona-tremia.
A new formulation of a saline
laxative, Visicol, that is useful to
prepare patients for procedures, was ap-proved for use in 2001. Each 2-g tablet
contains 1.102 g sodium phosphate monobasic monohydrate and 0.398 g sodium
phosphate dibasic anhydrous, for a total of 1.5 g sodium phosphate. Visicol
tablets, taken in two doses of 30 g approximately 12 hours apart, induce
di-arrhea that rapidly and effectively cleanses the entire colon. Each
administration has a purgative effect for approximately 1 to 3 hours.
Stimulant Cathartics
The stimulant cathartics
contain a variety of drugs whose exact mode of action is not known, although it
is thought that they act on the mucosa of the intestine to stimulate
peristalsis either by irritation or by exciting reflexes in the myenteric
plexuses. All act in the lumen of the GI tract and are inactive if given
parenterally. They produce irritation of the mucosa if given in large doses,
and this irritation affects water and ion transport. However, a direct local
irritation may not be essential to their action. It has been suggested that
these drugs may act by stimulating afferent nerves to initiate a reflex
in-crease in gut motility.
Anthraquinone derivatives
(e.g., cascara, aloe, senna, and rhubarb) are among the oldest laxatives known.
They act on the colon rather than on the ileum and produce evacuation 8 to 10
hours after administra-tion. This makes them particularly suitable for dosage
overnight. Cascara sagrada is one of the mildest of the
anthraquinone-containing laxatives.
Phenolphthalein is partially
absorbed (about 15% of a given dose) and excreted into the bile; hence, if it
is taken constantly, it will accumulate and exert too drastic an action. It
inhibits active sodium and glucose absorption in the bowel. Once widely
available in many over-the-counter products, it was pulled from the mar-ket
when it was linked to cancer.
Castor oil is a bland oil
that is hydrolyzed in the gut to yield ricinoleic acid, the active purging
agent. This hydrolysis requires bile, a fact that is sometimes over-looked when
castor oil is given as a laxative before ra-diography in biliary obstruction.
The ricinoleic acid acts on the ileum and colon to induce an increased fluid
se-cretion and colonic contraction.
Bisacodyl (Dulcolax) causes colonic contraction and
inhibits water absorption in the small and large intestine.
Isoosmotic Electrolyte Colonic Lavage Solutions
Electrolyte colonic lavage
solutions (e.g., GoLYTELY, Colyte, Nulytely) contain polyethylene
glycol and salts such as sodium
sulfate, sodium bicarbonate, sodium chloride, and potassium chloride in an
isoosmotic solu-tion. The dose is 4 L ingested over 2 to 4 hours either orally
or through a nasogastric tube. There is minimal net absorption or excretion of
fluid or electrolytes, and thus these are safe to use in patients with renal
insuffi-ciency. The patient has repeated liquid stools until the administered
solution has been expelled. If gastric emp-tying is slow, patients may have
abdominal distention with vomiting. This preparation should not be used if a
bowel obstruction or impaired gag reflex is present. It is used primarily to
clear the bowel before radiological or endoscopic procedures and occasionally
to assist with evacuation in a patient who has a sluggish colon.
Related Topics