Chapter: Medicine and surgery: Overdose, poisoning and addiction
Overview of acute poisoning - Overdose and poisoning
Overdose and poisoning
Overview of acute poisoning
Definition
Acute poisoning may result from accidental self-ingestion, deliberate self-harm or medical error.
Incidence/prevalence
Common presentation to A&E, commonest cause of medical admission of teenagers.
Age
Any, accidental ingestion most common in age 2–3 years.
Sex
Deliberate self-harm is more common in females.
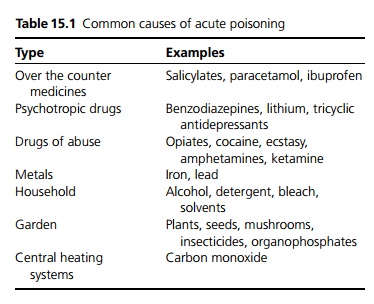
Aetiology
Many different substances are involved in poisoning, especially in children (see Table 15.1).
Clinical features
Acute poisoning should be considered in any patient presenting with altered levels of consciousness; however, the vast majority of patients who present are conscious. The patient or carers may be able to give a history and bring the containers or tablets. A full physical examination should be made.
· Central nervous system: Impaired consciousness, this can rapidly be assessed using the AVPU (Alert, responds to Voice, responds to Pain, Unresponsive) system or more formally using the Glasgow Coma scale.
· Other neurological features include altered behaviour, seizures, hallucinations, motor disturbances.
· Respiratory system: Altered respiration, halitosis.
· Cardiovascular system: Altered heart rate, arrhythmias, blood pressure instability.
· Gastrointestinal tract: Dry mouth, salivation, jaundice, vomiting and diarrhoea, alcohol may be smelt on the patient’s breath.
· Eyes: Miosis (constriction of the pupil is seen with opiates and organophosphates) or mydriasis (dilation of the pupil is seen with amphetamines, cocaine and tricyclic antidepressants), nystagmus.
· Ears: Tinnitus.
· Core temperature should be checked in unconscious patients.
Investigations
These will depend on the presentation and the availability of a reliable history. If this is not available the patient may have to be investigated and managed as an acute confusional state or coma. Appropriate investigations may include
· plasma paracetamol and salicylate levels.
· blood glucose.
· urine toxicology screen, there are immediate bed-side urine screening tests available for opiates, amphetamines, cocaine and cannabis.
· blood gases to detect respiratory failure or metabolic acidosis.
Complications
These depend on cause and clinical state but may include hypothermia, rhabdomyolysis and convulsions.
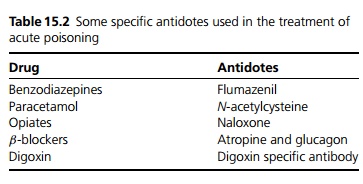
Management
If the patient is conscious, management is directed at the overdose itself. Specific information is available from the NPIS by phone or computer database available to NHS staff on the Internet (see also Table 15.2).
Principles of management:
· Reduction of absorption by emptying the stomach (vomiting or gastric lavage), if large quantities of drugs have been taken within the last hour. However, lavage or induced emesis is contraindicated following ingestion of corrosives, hydrocarbons or lipoid sub-stances. The patient must have an intact cough reflex or a cuffed endotracheal tube to protect the airway. Alternatively activated charcoal is useful for certain drugs, ideally within 4 hours of ingestion dependent on the drug.
· Active elimination may be used for certain poisons such as forced diuresis, exchange transfusion, peritoneal dialysis, haemodialysis, haemoperfusion.
· Care of the patient not only involves acute medical management, but also an investigation into the circumstances of the poisoning. Following an accidental overdose social circumstances need to be considered with regard to level of care. Patients presenting following deliberate ingestion require a psychiatric evaluation prior to discharge in order to assess their risk of further self-harm and to identify and manage any underlying precipitants for the overdose.
Related Topics