Chapter: Psychiatric Mental Health Nursing : Somatoform Disorders
Overview of Somatoform Disorders
OVERVIEW OF SOMATOFORM DISORDERS
Somatization is defined as the
transference of mental experiences
and states into bodily symptoms. Somatoform
disorders can be characterized as
the presence of physical symptoms
that suggest a medical condition without a demonstrable organic basis to
account fully for them. The three central features of somatoform disorders are
as follows:
·
Physical complaints suggest major medical illness but have no
demonstrable organic basis.
·
Psychologic factors and conflicts seem important in ini-tiating,
exacerbating, and maintaining the symptoms.
·
Symptoms or magnified health concerns are not under the client’s
conscious control (Hollifield, 2005).
Clients are convinced they harbor serious physical problems despite
negative results during diagnostic test-ing. They actually experience these
physical symptoms as well as the accompanying pain, distress, and func-tional
limitations such symptoms induce. Clients do not willfully control the physical
symptoms. Although their illnesses are psychiatric in nature, many clients do
not seek help from mental health professionals. Unfortunately, many health care
professionals who do not understand the nature of somatoform disorders are not
sympathetic to these clients’ complaints (Andreasen & Black, 2006). Nurses
must remember that these clients really experi-ence the symptoms they describe
and cannot voluntarily control them.
The five specific somatoform disorders are as follows (American
Psychiatric Association [APA], 2000):
·
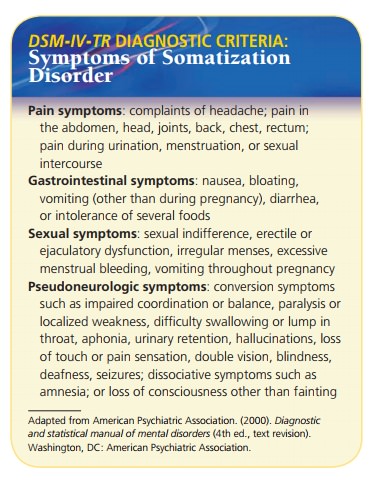
Somatization disorder is characterized by multiple physical symptoms. It begins by 30
years of age, ex-tends over several years, and includes a combination of pain
and gastrointestinal, sexual, and pseudoneurologic symptoms.
·
Conversion disorder, sometimes called conversion
re-action, involves unexplained, usually sudden deficits in sensory or motor
function (e.g., blindness, paralysis). These deficits suggest a neurologic
disorder but are associated with psychologic factors. An attitude of la
belle
indifférence, a seeming lack of concern or distress, is
a key feature.
·
Pain disorder has the primary physical
symptom of pain, which generally is
unrelieved by analgesics and greatly affected by psychologic factors in terms
of onset, severity, exacerbation, and maintenance.
·
Hypochondriasis is preoccupation with the
fear that one has a serious disease
(disease conviction) or will get a
serious disease (disease phobia). It
is thought that clients with this disorder misinterpret bodily sensations or
functions.
·
Body dysmorphic disorder is preoccupation with an imagined or exaggerated defect in
physical appearance such as thinking one’s nose is too large or teeth are
crooked and unattractive.
Somatization disorder, conversion disorder, and pain dis-order are
more common in women than in men; hypochon-driasis and body dysmorphic disorder
are distributed equally by gender. Somatization disorder occurs in 0.2% to 2%
of the general population. Conversion disorder occurs in less than 1% of the population.
Pain disorder is commonly seen in medical practice, with 10% to 15% of people
in the United States reporting work disability related to back pain alone (APA,
2000). Hypochondriasis is estimated to occur in 4% to 9% of people seen in
general medical practice. No statistics of the incidence of body dysmorphic
disorder are available.
Related Topics