Chapter: Psychiatric Mental Health Nursing : Somatoform Disorders
Application of the Nursing Process - Somatoform Disorders
APPLICATION OF THE NURSING
PROCESS
The underlying mechanism of somatization is consistent for clients
with somatoform disorders of all types. This section discusses application of
the nursing process for cli-ents with somatization; differences among the
disorders are highlighted in the appropriate places.
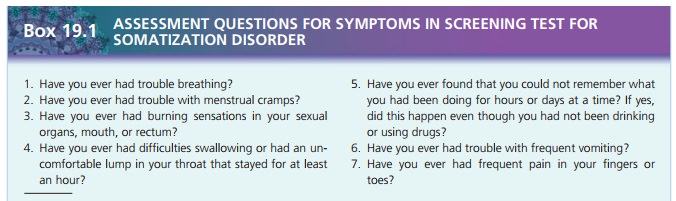
Assessment
The nurse must investigate physical health status thoroughly to
ensure there is no underlying pathology requiring treatment. When a client has
been diagnosed with a somatoform disorder, it is important not to dismiss all
future complaints because at any time the client could develop a physical
condition that would require medical attention.
History
Clients usually provide a lengthy and detailed account of previous
physical problems, numerous diagnostic tests, and perhaps even a number of
surgical procedures. It is likely that they have seen multiple health care
providers over several years. Clients may express dismay or anger at the
medical community with comments such as “They just can’t find out what’s wrong
with me” or “They’re all incom-petent, and they’re trying to tell me I’m
crazy!” The excep-tion may be clients with conversion disorder, who show little
emotion when describing physical limitations or lack of a medical diagnosis (la belle indifférence).
General Appearance and Motor Behavior
Overall appearance usually is not remarkable. Often, cli-ents walk
slowly or with an unusual gait because of the pain or disability caused by the
symptoms. They may exhibit a facial expression of discomfort or physical
dis-tress. In many cases, they brighten and look much better as the assessment
interview begins because they have the nurse’s undivided attention. Clients
with somatization dis-order usually describe their complaints in colorful,
exag-gerated terms but often lack specific information.
Mood and Affect
Mood is often labile, shifting from seeming depressed and sad when
describing physical problems to looking bright and excited when talking about
how they had to go to the hospital in the middle of the night by ambulance.
Emo-tions are often exaggerated, as are reports of physical symptoms. Clients
describing a series of personal crises related to their physical health may
appear pleased rather than distressed about these situations. Clients with
con-version disorder display an unexpected lack of distress.
Thought Process and Content
Clients who somatize do not experience disordered thought
processes. The content of their thinking is pri-marily about often exaggerated
physical concerns; for example, when they have a simple cold, they may be
con-vinced it is pneumonia. They may even talk about dying and what music they
want played at their funeral.
Clients are unlikely to be able to think about or to respond to
questions about emotional feelings. They will answer questions about how they
feel in terms of physical health or sensations. For example, the nurse may ask,
“How did you feel about having to quit your job?” The cli-ent might respond,
“Well, I thought I’d feel better with the extra rest, but my back pain was just
as bad as ever.”
Clients with hypochondriasis focus on the fear of seri-ous illness
rather than the existence of illness, as seen in clients with other somatoform
disorders. However, they are just as preoccupied with physical concerns as
other somatizing clients and are likewise very limited in their abilities to
identify emotional feelings or interpersonal issues. Clients with
hypochondriasis are preoccupied with bodily functions, ruminate about illness,
are fascinated with medical information, and have unrealistic fears about
potential infection and prescription medication.
Sensorium and Intellectual Processes
Clients are alert and oriented. Intellectual functions are
unimpaired.
Judgment and Insight
Exaggerated responses to their physical health may affect clients’
judgment. They have little or no insight into their behavior. They are firmly
convinced their problem is entirely physical and often believe that others
don’t understand.
Self-Concept
Clients focus only on the physical part of themselves. They are
unlikely to think about personal characteristics or strengths and are
uncomfortable when asked to do so. Cli-ents who somatize have low self-esteem
and seem to deal with it by totally focusing on physical concerns. They lack
confidence, have little success in work situations, and have difficulty
managing daily life issues, which they relate solely to their physical status.
Roles and Relationships
Clients are unlikely to be employed, although they may have a past
work history. They often lose jobs because of excessive absenteeism or
inability to perform work; clients may have quit working voluntarily because of
poor physi-cal health. Consumed with seeking medical care, they have difficulty
fulfilling family roles. It is likely that these cli-ents have few friends and
spend little time in social activi-ties. They may decline to see friends or to
go out socially for fear that they would become desperately ill away from home.
Most socialization takes place with members of the health care community.
Clients may report a lack of family support and under-standing.
Family members may tire of the ceaseless com-plaints and the client’s refusal
to accept the absence of a medical diagnosis. The illnesses and physical
conditions often interfere with planned family events such going on vacations
or attending family gatherings. Home life is often chaotic and unpredictable.
Physiologic and Self-Care Concerns
In addition to the multitude of physical complaints, these clients
often have legitimate needs in terms of their health practices. Clients who
somatize often have sleep pattern disturbances, lack basic nutrition, and get
no exercise. In addition, they may be taking multiple pre-scriptions for pain
or other complaints. If a client has been using anxiolytics or medications for
pain, the nurse must consider the possibility of withdrawal  .
.
Data Analysis
Nursing diagnoses commonly used when working with clients who
somatize include the following:
·
Ineffective Coping
·
Ineffective Denial
·
Impaired Social Interaction
·
Anxiety
·
Disturbed Sleep Pattern
·
Fatigue
·
Pain
Clients with conversion disorder may be at risk for disuse syndrome
from having pseudoneurologic paralysis symptoms. In other words, if clients do
not use a limb for a long time, the muscles may weaken or atrophy from lack of
use.
Outcome Identification
Treatment outcomes for clients with a somatoform disor-der may
include the following:
·
The client will identify the relationship between stress and
physical symptoms.
·
The client will verbally express emotional feelings.
·
The client will follow an established daily routine.
·
The client will demonstrate alternative ways to deal with stress,
anxiety, and other feelings.
The client will demonstrate healthier behaviors regard-ing rest,
activity, and nutritional intake.
Intervention
Providing Health Teaching
The nurse must help the client learn how to establish a daily
routine that includes improved health behaviors. Adequate nutritional intake,
improved sleep patterns, and a realistic balance of activity and rest are all
areas with which the client may need assistance. The nurse should expect
resistance, including protests from the client that she or he does not feel
well enough to do these things. The challenge for the nurse is to validate the
client’s feelings while encouraging her or him to participate in activities.
Nurse: “Let’s take a walk outside for some fresh air.” (encouraging collaboration)
Client: “I wish I could, but I feel so terrible, I just can’t do it.”
Nurse: “I know this is difficult, but some exer-cise is essential. It
will be a short walk.” (validation; encourag-ing collaboration)
The nurse can use a similar approach to gain client participation
in eating more nutritious foods, getting up and dressed at a certain time every
morning, and setting a regular bedtime. The nurse also can explain that
inactivity and poor eating habits perpetuate discomfort and that often it is
necessary to engage in behaviors even when one doesn’t feel like it.
Client: “I just can’t eat anything. I have no appetite.”
Nurse: “I know you don’t feel well, but it is important to begin eating.” (validation;
encour-aging collaboration)
Client: “I promise I’ll eat just as soon as I’m hungry.”
Nurse: “Actually, if you begin to eat a few bites, you’ll begin to feel better, and your appetite may improve.” (encouraging collaboration)
The nurse should not strip clients of their somatizing defenses
until adequate assessment data are collected and other coping mechanisms are
learned. The nurse should not attempt to confront clients about somatic
symptoms or attempt to tell them that these symptoms are not “real.” They are
very real to clients, who actually experience the symptoms and associated
distress.
Assisting the Client to Express Emotions
Teaching about the relationship between stress and physi-cal
symptoms is a useful way to help clients begin to see the mind–body
relationship. Clients may keep a detailed journal of their physical symptoms.
The nurse might ask them to describe the situation at the time such as whether
they were alone or with others, whether any disagreements were occurring, and
so forth. The journal may help clients to see when physical symptoms seemed
worse or better and what other factors may have affected that perception.
Limiting the time that clients can focus on physical complaints
alone may be necessary. Encouraging them to focus on emotional feelings is
important, although this can be difficult for clients. The nurse should provide
attention and positive feedback for efforts to identify and discuss feelings.
It may help for the nurse to explain to the family about primary
and secondary gains. For example, if the family can provide attention to
clients when they are feeling better or fulfilling responsibilities, clients
are more likely to continue doing so. If family members have lavished attention
on clients when they have physical complaints, the nurse can encourage the
relatives to stop reinforcing the sick role.
Teaching Coping Strategies
Two categories of coping strategies are important for cli-ents to
learn and to practice: emotion-focused
coping strategies, which help
clients relax and reduce feelings of
stress, and problem-focused coping
strategies, which help to resolve or change a client’s behavior or situation
or manage life stressors. Emotion-focused strategies include progressive
relaxation, deep breathing, guided imagery, and distractions such as music or
other activities. Many approaches to stress relief are available for clients to
try. The nurse should help clients to learn and practice these techniques,
emphasizing that their effectiveness usually improves with routine use. Clients
must not expect such techniques to eliminate their pain or physical symptoms;
rather, the focus is helping them to manage or diminish the intensity of the
symptoms.
Problem-focused coping strategies include learning problem-solving
methods, applying the process to identi-fied problems, and role-playing
interactions with others. For example, a client may complain that no one comes
to visit or that she has no friends. The nurse can help the client to plan
social contact with others, can role-play what to talk about (other than the
client’s complaints), and can improve the client’s confidence in making
relationships. The nurse also can help clients to identify stressful life
situations and plan strategies to deal with them. For example, if a client
finds it difficult to accomplish daily household tasks, the nurse can help him
to plan a schedule with difficult tasks followed by something the client may
enjoy.
Evaluation
Somatoform disorders are chronic or recurrent, so changes are
likely to occur slowly. If treatment is effective, the client should make fewer
visits to physicians as a result of physical complaints, use less medication
and more positive coping techniques, and increase functional abilities.
Improved fam-ily and social relationships are also a positive outcome that may
follow improvements in the client’s coping abilities.
Related Topics