Chapter: Modern Pharmacology with Clinical Applications: Antianginal Drugs
Organic Nitrates Antianginal Drugs
SPECIFIC
ANTIANGINAL DRUGS
Organic Nitrates
Organic nitrates have been
used in the therapy of angina pectoris routinely for more than 140 years, and
their use is increasingly favored in a variety of other cardiac conditions,
such as decompensated congestive heart failure and acute myocardial infarction.
The pro-totype of these agents is nitroglycerin. Other common organic nitrates
are isosorbide mononitrate (Ismo),
isosorbide dinitrate (Isordil, Sorbitrate)
and pentaery-thritol tetranitrate (Peritrate).
With the exception of ni-troglycerin, which is a liquid having a high vapor
pres-sure, these compounds are solid at room temperature. All organic nitrates
are very lipid soluble.
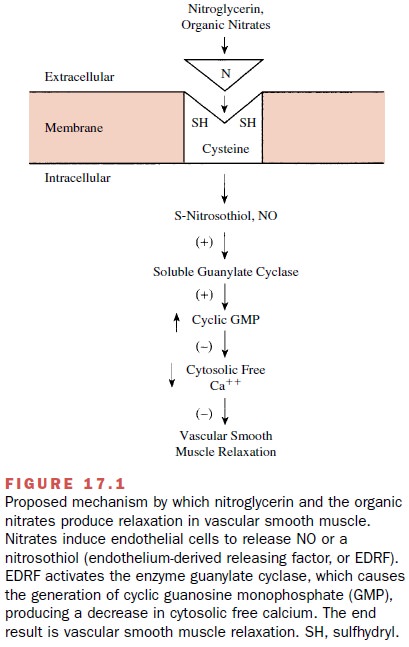
Mechanism of Vasodilator Action
The mechanism of action of
nitroglycerin and other or-ganic nitrates is thought to involve an interaction
with nitrate receptors that are present in vascular smooth muscle. Intact
vascular endothelium is not necessary for the vasodilator action of the
nitrates to be produced. The nitrate receptor possesses sulfhydryl groups,
which reduce nitrate to inorganic nitrite and nitric oxide (NO). The formation
of nitrosothiols, and possibly free NO, has been proposed to stimulate
intracellular solu-ble guanylate cyclase, which leads to an increase in
in-tracellular cyclic guanosine monophosphate (GMP) formation (Fig. 17.1). The
increase in GMP results in vascular smooth muscle relaxation, possibly through
in-hibition of calcium entry via L-type calcium channels, decreased calcium
release from the sarcoplasmic reticu-lum, or via an increase in calcium
extrusion via a sar-colemmal Ca++ -adenosine triphosphatase
(ATPase).
Absorption, Metabolism, and Excretion
Nitroglycerin is a lipid-soluble substance that is rapidly absorbed across the sublingual or buccal mucosa. Its on-set of action occurs within 2 to 5 minutes, with maximal effects observed at 3 to 10 minutes. Little residual activ-ity remains 20 to 30 minutes after sublingual adminis-tration.
The plasma half-life of nitroglycerin, given sublingually or by spray, is
estimated to be 1 to 3 min-utes. Isosorbide dinitrate and pentaerythritol
tetrani-trate also can be administered sublingually or buccally. These
compounds have a slower onset and slightly longer duration of action than
sublingually or buccally administered nitroglycerin.
Nitroglycerin and other
organic nitrate esters un-dergo first-pass metabolism and are rapidly
metabo-lized in the liver by the enzyme glutathione organic nitrate reductase.
Although the metabolites of nitro-glycerin are virtually inactive as
vasodilators, two metabolites of isosorbide dinitrate, isosorbide 2-mononitrate
and isosorbide 5-mononitrate, do retain some vasodilator and antianginal
activity. Isosorbide mononitrate can be administered orally and does not
undergo any first-pass metabolism. The latter esters and their metabolites are
water soluble and are readily ex-creted by the kidney.
Pharmacological Actions
There is little doubt
concerning the effectiveness of ni-troglycerin in the treatment of angina
pectoris. However, the exact mechanism by which the drug acts to reduce
myocardial ischemia is still controversial (Fig. 17.2). Although nitroglycerin
dilates both peripheral ca-pacitance and resistance vessels, the effect on the
ve-nous capacitance system predominates. Dilation of the capacitance vessels
leads to pooling of blood in the veins and to diminished venous return to the
heart (de-creased preload). This reduces ventricular diastolic vol-ume and
pressure and shifts blood from the central to the peripheral compartments of
the cardiovascular sys-tem. These effects of nitroglycerin and other organic
ni-trates are similar to those of mild phlebotomy, which has been shown
clinically to relieve acute anginal at-tacks by decreasing circulating blood
volume.
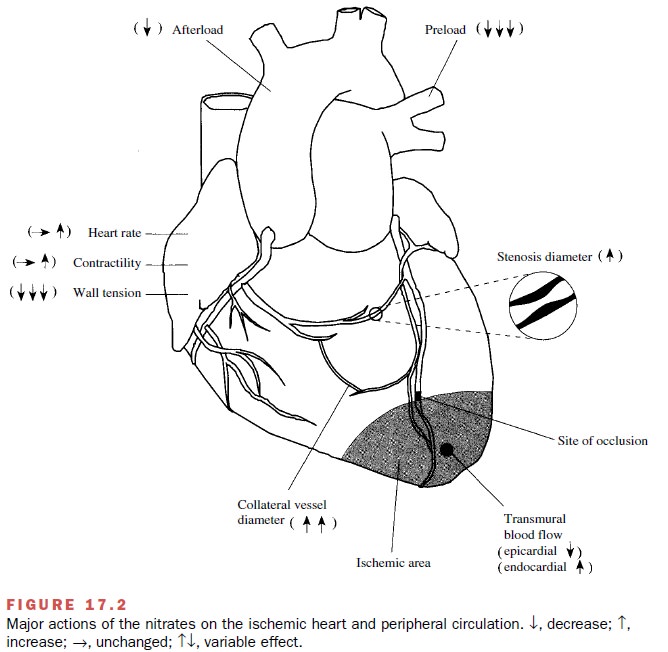
According to Laplace’s law, a reduction in ventricu-lar pressure and heart size results in a decrease in the myocardial wall tension that is required to develop a given intraventricular pressure and therefore decreases oxygen requirement. Since blood flow to the subendo-cardium occurs primarily in diastole, the reduction in left ventricular end diastolic pressure induced by nitro-glycerin reduces extravascular compression around the subendocardial vessels and favors redistribution of coronary blood flow to this area.
This effect of nitro-glycerin on the distribution of coronary flow is
impor-tant because the subendocardium is particularly vulner-able to ischemia
during acute anginal attacks.
At higher concentrations,
nitroglycerin also relaxes arteriolar smooth muscle, which leads to a decrease
in both peripheral vascular resistance and aortic imped-ance to left
ventricular ejection (decreased afterload). The decreased resistance to
ventricular ejection may also reduce myocardial wall tension and oxygen
re-quirements.
Thus, nitroglycerin relieves
the symptoms of angina by restoring the balance between myocardial oxygen
supply and demand. Oxygen demand is lowered as a consequence of the reduction
in cardiac preload and af-terload, and this results in a decrease in myocardial
wall tension. Oxygen supply to the subendocardium of isch-emic areas is
increased because extravascular compres-sion around the subendocardial vessels
is reduced. In addition, nitroglycerin may increase blood flow to isch-emic
areas by its direct vasodilator effect on eccentric epicardial coronary artery
stenoses and collateral blood vessels and by its action to inhibit platelet
aggregation. Other organic nitrates are thought to exert the same beneficial
actions as nitroglycerin.
Nitrate-induced Late Preconditioning
Recent findings suggest a
potential new action of ni-trates in the treatment of patients with ischemic
heart disease. Administration of intravenous (IV) or trans-dermal nitroglycerin
to conscious rabbits exerts a pro-tective effect against myocardial infarction
that persists for 72 hours; this effect has been termed late precondi-tioning.
The magnitude of this effect was also found to persist in animals that
displayed tolerance to the vascu-lar effects of nitroglycerin. Although this
effect of nitro-glycerin has not been demonstrated unequivocally in patients
receiving long-term nitrate therapy, these re-sults are provocative and may
support new uses of ni-trates in patients or benefits that have until now
re-mained unrecognized.
Clinical Uses
Sublingual or buccal nitroglycerin
is used either to ter-minate an acute attack of angina or for short-term
pre-vention of angina. Nitroglycerin is also the mainstay of therapy for
relieving acute coronary vasospasm because of its rapid onset of action. When
taken at the onset of chest pain, the effects of nitroglycerin appear within 2
to 5 minutes; however, the true duration of action is diffi-cult to establish
in patients with secondary angina, since the onset of pain causes patients to
reduce their physi-cal activity, and this alone can ameliorate the symptoms.
Isosorbide dinitrate and pentaerythritol tetranitrate also can be taken
sublingually, shortly before antici- pated physical or emotional stress, to
prevent anginal attacks.
Nitroglycerin ointment
applied to the skin acts within 15 minutes and may produce its effects for 2 to
6 hours. Sustained-release transdermal nitroglycerin has been shown to deliver
an antianginal effect for 2 to 4 hours following small doses and up to 24 hours
after larger doses.
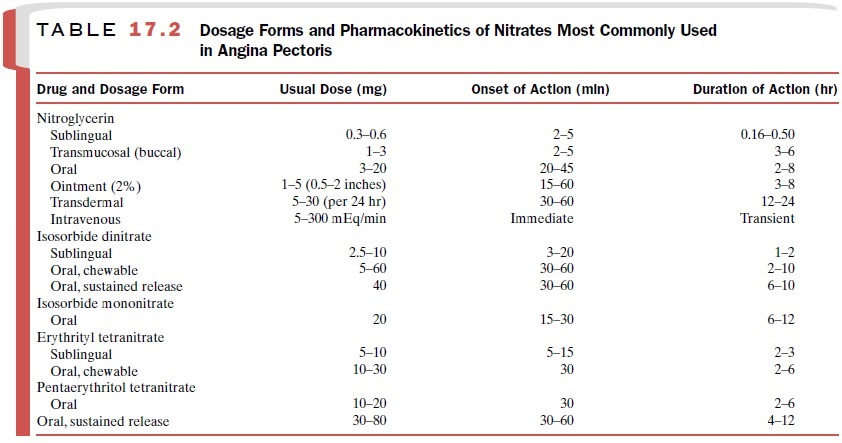
Orally administered long-acting
nitrates, including nitroglycerin and various nitrate esters, nitroglycerin
ointment, and transdermal nitroglycerin, were devel-oped with the goal of
providing a nitrate preparation that would have prolonged pharmacological
activity for prophylactic therapy of angina pectoris. Considerable controversy
surrounds the therapeutic use of the orally active agents because of their
extensive first-pass me-tabolism, and many clinicians consider them to be
inef-fective. More recently, however, numerous clinical in-vestigations have
demonstrated the efficacy of transdermal nitroglycerin, although tolerance can
be a problem with prolonged transdermal exposure to nitro-glycerin. The drugs
and dosage forms of organic nitrates available for therapeutic use, their usual
dose, onset of action, and duration of action are summarized in Table 17.2.
Tolerance and Dependence
Repeated and frequent
exposure to organic nitrates is accompanied by the development of tissue
tolerance to the drug’s vasodilating effects. When nitroglycerin for-mulations
(e.g., transdermal patches, sustained-release oral dosing, or ointments) that
produce sustained plasma and tissue levels are used, tolerance may occur within
24 hours. The mechanism underlying the phe-nomenon of nitrate tolerance is not
as yet completely understood but may be related to a nitrate-induced ox-idation
of sulfhydryl groups via the formation of free radicals, a decrease in the
sensitivity of vascular smooth muscle soluble guanylate cyclase, or activation
of the renin–angiotensin system.
To help avoid nitrate
tolerance, clinicians should employ the smallest effective dose and administer
the compound infrequently. A daily nitrate-free period is also recommended,
particularly with use of the trans-dermal patches or ointment. A better
understanding of the pharmacokinetic profile achieved with these
sus-tained-release formulations should result in more effec-tive dosing
regimens.
Since depletion of tissue stores of sulfhydryl groups has been proposed to play an important role in nitrate tolerance, some investigators have administered sulfhydryl-containing compounds in an attempt to re-verse or prevent the development of tolerance. The most commonly used agent is N-acetylcysteine (NAC), which is hydrolyzed in vivo to cysteine.
Although some investigators have shown a
positive effect with NAC, the antinitrate tolerance effect of this compound has
not been universally confirmed. Thus, further well-controlled clinical studies
are necessary to establish the effectiveness of sulfhydryl-containing compounds
at preventing or reversing nitrate tolerance.
Industrial exposure to
organic nitrates induces both tolerance and physical dependence. The state of
de-pendence becomes manifest when exposure to nitrates is withdrawn suddenly.
For example, munitions workers who have become dependent on nitroglycerin have
been reported to undergo angina, myocardial infarc-tion, or even sudden death
following removal from contact with nitroglycerin. Some of these patients
showed symptoms of ischemic heart disease, even though their coronary
arteriography was judged to be normal. Since it is possible that coronary
vasospasm plays a role in the pathogenesis of angina that occurs in
nitrate-dependent individuals, these patients should be cautioned to watch for
increased chest pain when they withdraw from medication or discontinue their
exposure.
Adverse Effects
Vascular headache, postural
hypotension, and reflex tachycardia are common side effects of organic nitrate
therapy. Fortunately, tolerance to nitrate-induced head-ache develops after a
few days of therapy. Postural hy-potension and tachycardia can be minimized by
proper dosage adjustment and by instructing the patient to sit down when taking
rapidly acting preparations. An ef-fective dose of nitrate usually produces a
fall in upright systolic blood pressure of 10 mm Hg and a reflex rise in heart
rate of 10 beats per minute. Larger changes than these should be avoided,
because a reduction in myo-cardial perfusion and an increase in cardiac oxygen
re-quirements may actually exacerbate the angina.
Since nitrite ions oxidize
the iron atoms of hemo-globin and convert it to methemoglobin, there may be a
loss in oxygen delivery to tissues. While methemoglo-binemia does not follow
therapeutic doses of organic ni-trates, it can be observed after overdosage or
accidental poisoning.
Cautions
Chest pain that is not
relieved by two or three tablets within 30 minutes may be due to an acute
myocardial infarction. In addition, nitrate administration may result in an
increase in intracranial pressure, and therefore, these drugs should be used
cautiously in patients with cerebral bleeding and head trauma.
Related Topics