Chapter: Nutrition and Diet Therapy: Diet and Diabetes Mellitus
Nutritional Management for Diabetes Mellitus
NUTRITIONAL MANAGEMENT
The dietitian will
need to know the client’s diet history, food likes and dislikes, and lifestyle
at the onset. The client’s calorie needs will depend on age, activi-ties, lean
muscle mass, size, and REE.
It is recommended that
carbohydrates provide 50% to 60% of the calories.
Approximately 40% to
50% should be from complex carbohydrates (starches).
The remaining 10% to
20% of carbohydrates could be from simple sugar.
Research provides no
evidence that carbohydrates from simple sugars are digested and absorbed more
rapidly than are complex carbohydrates, and they do not appear to affect blood
sugar control. It is the total amount of
carbo-hydrates eaten that affects blood sugar levels rather than the type.
Being able tosubstitute foods containing sucrose for other carbohydrates
increases flexibility in meal planning for the diabetic.
Fats should be limited
to 30% of total calories, and proteins should provide from 15% to 20% of total
calories. Lean proteins are advisable because they contain limited amounts of
fats.
Regardless of the
percentages of energy nutrients prescribed, the foods ultimately eaten should
provide sufficient vitamins and minerals as well as energy nutrients.
The client with type 1
diabetes needs a nutritional plan that balances calories and nutrient needs
with insulin therapy and exercise. It is important that meals and snacks be
composed of similar nutrients and calories and eaten at regular times each day.
Small meals plus two or three snacks may be more helpful in maintaining steady
blood glucose levels for these clients than three large meals each day.
The client with type 1
diabetes should anticipate the possibility of missing meals occasionally and
carry a few crackers and some cheese or peanut butter to prevent hypoglycemia,
which can occur in such a circumstance.
The client with type 2
diabetes may be overweight. The nutritional goal for this client is not only to
keep blood glucose levels in the normal range but to lose weight as well.
Exercise can help attain both goals.
Carbohydrate Counting
Carbohydrate counting is the newest method for teaching a diabetic client how
to control blood sugar
with food. The starch and bread category, milk, and fruits have all been put
under the heading of “carbohydrates.” This means that these three food groups
can be interchanged within one meal. One would still have the same number of
servings of carbohydrates, but it would not be the typical number of starches
or fruits and milk that one usually eats. For example, one is to have four
carbohydrates for breakfast (2 breads, 1 fruit, and 1 milk). If there is no
milk available, a bread or fruit must be eaten in place of the milk. The
exchangelists are utilized in carbohydrate counting as well as in traditional
meal planning. Protein, approximately 3 to 4 ounces, is eaten for lunch and
dinner. One or two fat exchanges are recommended for each meal. Two
carbohydrates should be eaten for an evening snack. These are only beginning
guidelines. A dietitian or diabetic educator can help tailor this to the
individual client.
Diets Based on Exchange Lists
The method of diet
therapy most commonly used for diabetic clients is that based on exchange lists. These lists were
developed by the American Diabetes Association in conjunction with the American
Dietetic Association and are summarized in Table 17-2 and included completely
in Table 17-3.
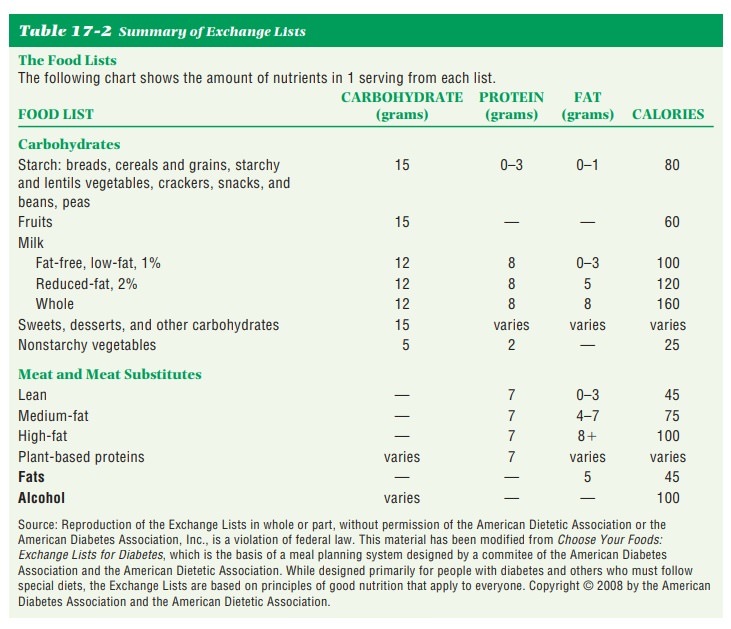
Under this plan, foods
are categorized by type and included in the lists in Table 17-3.
The
foods within each list contain approximately equal amounts of calo-ries,
carbohydrates, protein, and fats. This means that any one food on a particular
list can be substituted for any other food on that particular list and still pro-vide the client with the prescribed
types and amounts of nutrients and calories.
The
amounts of nutrients and calories on one list are not the same as those on any
other list. Each list includes serving size by volume or weight and the calorie
value of each food item, in addition to the grams of carbohydrates, and, when
appropriate, proteins and fats. The number of calories needed will determine
the number of items prescribed from any particular list. These lists also can
be used to control calorie content of diets and are thus appropriate for
low-calorie diets.
The
total energy requirements for adult diabetic clients who are not overweight
will be the same as for nondiabetic individuals. When clients are overweight, a
reduction in calories will be built into the diet plans, typically allowing for
a weight loss of 1 pound a week.
The
diet is given in terms of exchanges rather than as particular foods. For
example, the menu pattern for breakfast may include 1 fruit exchange, 1 meat
exchange, 2 bread exchanges, and 2 fat exchanges. The client may choose the
desired foods from the exchange lists for each meal but must adhere to the
specific exchange lists named and the specific number of exchanges on each
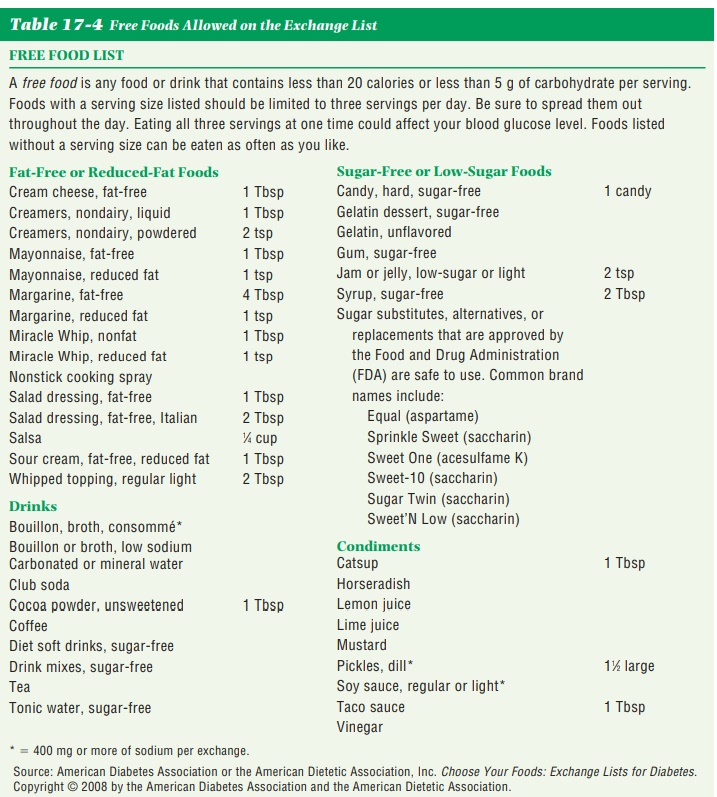
list. Vegetables (nonstarchy) are relatively free and can be eaten in amounts
up to 11⁄2 cups cooked or 3 cups raw. If more than this amount is
eaten at one meal, count the additional amount as one more carbohydrate. Snacks
are built into the plan. In this way, the client has variety in a simple yet
controlled way.
When there are changes
in one’s physical condition, such as pregnancy or lactation, or in one’s
lifestyle, the diet will need to be modified. A change in job or in working
hours can affect nutrient and calorie requirements. When such changes occur,
the client should be advised to consult her or his physi-cian or dietitian so
that calorie and insulin needs can be promptly adjusted.
Related Topics