Chapter: Introduction to Human Nutrition: Food and Nutrition-Related Diseases: The Global Challenge
Nutrition-related diseases in developed countries
Nutrition-related diseases in developed countries
The current situation
Economic development, education, food security, and access to health care and immunization programs in developed countries have resulted in dramatic decreases in undernutrition-related diseases. Un-fortunately, many of these factors have also led to unhealthy behaviors, inappropriate diets, and lack of physical activity, which has exacerbated the develop-ment of chronic diseases, also known as noncommu-nicable diseases (NCDs). These NCDs are now the main contributors to the health burden in developed countries (these are countries with established market economies).
In 2002, 28.2 million global deaths (58.6%) were from NCDs. In the same year the predicted mortality for 2020 was 49.6 million (72.6% of all deaths). This is an increase from 448 to 548 deaths per 100,000, despite an overall downward trend in mortality rates. Although the burden will fall increasingly on developing countries NCDs remain the major cause of death in developed countries.
Definition, terminology and characteristics
The NCDs that are related to diet and nutrient intakes are obesity, hypertension, atherosclerosis, ischemic heart disease, myocardial infarction, cerebrovascular disease, stroke, diabetes mellitus (type 2), osteoporo-sis, liver cirrhosis, dental caries, and nutrition-induced cancers of the breast, colon, and stomach. They develop over time in genetically susceptible individu-als because of exposure to interrelated societal, behavioral, and biological risk factors. Together with tobacco use, alcohol abuse, and physical inactivity, an unhealthy or inappropriate diet is an important modifiable risk factor for NCDs. Diet, therefore, plays a major role in prevention and treatment of NCDs. NCDs are sometimes called “chronic diseases,” but some infectious diseases such as HIV/AIDS and tuberculosis are also chronic. They have also been called “diseases of affluence,” which is a misnomer because in developed, affluent countries, they are more common in lower socioeconomic groups. Some scientists have a problem with the term “noncom-municable” because lifestyles, including diets, are transferable between populations. The term “non-communicable” should therefore be seen as no transfer of an infectious agent from one organism to another. Because of its first emergence in “Westernized” societies and associations with Western lifestyles, it is often called “Western” diseases, also a misnomer. It is becoming more prevalent in developing countries in other parts of the world. Another misconception is that it is a group of diseases affecting only older people. The risk factors for NCDs accumulate throughout the life course – from infancy to adult-hood, and manifest after decades of exposure. The increase in childhood obesity is especially of concern because it has long-term implications for NCDs in the developed world.
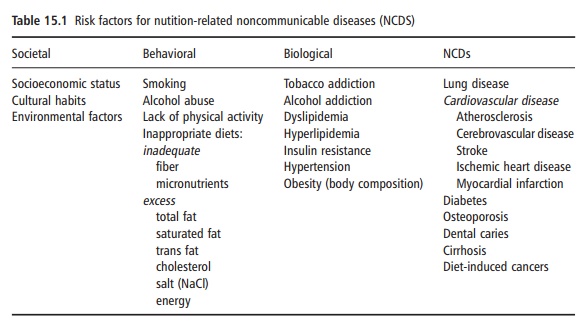
Risk factors for NCDs
Table 15.1 lists the risk factors for NCDs. The factors are interrelated and form a chain of events starting with societal factors such as socioeconomic status and environments that influence behavior, leading to the development of biological risk factors that cause the NCDs. The biological risk factors often cluster together. For example, obesity (abnormal body com-position) is associated with insulin resistance, hyper-lipidemia, and hypertension, which all contribute to the development of both cardiovascular disease and diabetes. Cardiovascular disease is furthermore one of the complications of untreated diabetes.
The role of nutrition
The evidence that diets and specific nutrient deficien-cies and excesses influence the development of NCDs and may therefore be used in prevention and treatment is solid. It comes from extensive research which collec-tively gave convincing evidence of the relationships between nutrition and NCDs: first, from ecological studies which compared different populations, the effects of migration of populations, food availability during economic development, and differences in dietary and nutrient intakes. Second, numerous epide-miological studies have established the associations between diet and biological risk factors of NCDs. Third, interventions with specific nutrients and foods in placebo-controlled trials using both healthy and dis-eased subjects confirmed the relationships seen in epi-demiological studies. And last, molecular and genetic research has elucidated many mechanisms through which diet and nutrients affect genetic mutation and expression, adding to our knowledge of how nutrition influences NCD development. This body of knowledge has led to several sets of international dietary recom-mendations and guidelines to reduce the burden of nutrition-related NCDs.
Prevention of NCDs in developed countries
The complex chain of events where behavioral and lifestyle factors influence the development of the bio-logical risk factors for NCDs, emphasizes the need for a multisectorial approach in which all factors in the chain are targeted throughout the life course. In addi-tion to the medical treatment of some biological risk factors (such as pharmacological treatment of hyper-cholesterolemia) and of the NCD itself (such as blood glucose control in diabetes) there is convincing evidence that primary prevention is possible, cost-effective, affordable, and sustainable. In the developed world, early screening and diagnosis, and access to health care make primary prevention more feasible than in many developing countries. However, over-coming the barriers to increase physical activity and changing dietary behavior towards more prudent, low-fat, high-fiber diets may be more difficult. The strategies and programs to prevent NCDs would be similar in developed and developing countries, although the context and specific focus of different interventions may vary. Because the future burden of NCDs will be determined by the accumulation of risks over a lifetime, the life course approach is rec-ommended. This will include optimizing the nutri-tional status of pregnant women, breastfeeding of infants, ensuring optimal nutrition status and growth of children, preventing childhood obesity and promoting “prudent” diets for adoles-cents, adults, and older people. Addressing childhood obesity in developed countries is one of the biggest nutritional challenges these countries is facing today. Increases in the prevalence of childhood obesity have been documented for most developed countries. In the USA, the National Health and Nutrition Examination Surveys (NHANES) showed substantial increases over the last two decades in overweight and obese children aged 2–19 years. More than 15% of American children are currently considered obese. The International Obesity Task Force estimates that at least 22 million of the world’s children under 5 years of age are overweight or obese. Overweight and obesity have dire consequences in children. These children already display many of the other biological risk factors of NCDs. There are also immediate health consequences such as risks to develop gallstones, hep-atitis, sleep apnea, and others. Moreover, these chil-dren have a lack of self-esteem, are often stigmatized and have difficulties with body image and mobility. Overweight and obese children often become over-weight or obese adults and carry the long-term risk of premature morbidity and mortality from NCDs. Children in the developed world are exposed to a food environment in which high energy-dense and micro-nutrient-poor foods, beverages, and snacks are avail-able, affordable, and aggressively marketed. This illustrates that to address the problem of childhood obesity, active and responsible partnerships and common agendas should be formed between all stakeholders (for example between governments, NGOs and the food industry). There are indications that dialogue with the food industry is not sufficient, and that many countries are now considering or already implementing legislation to create a more healthy food environment for children. The problems of childhood overweight and obesity and consequent increases in NCDs are not only seen in developed countries. They are emerging in developing countries and in some the total number of children affected exceeds those in developed countries. Timely inter-ventions are needed to prevent the escalation experi-enced in developed countries.
Related Topics