Chapter: Essentials of Psychiatry: Childhood Disorders: Mental Retardation
Mental Retardation: Evaluation of Clinical Data, Aggression
Evaluation of Clinical Data
The clinical observations should be interpreted in
light of a pa-tient’s life experiences, learning, understanding and
communica-tion level. The global IQ or overall mental age alone is not a good
guide here. In particular, the psychiatrist should:
· Assess
clinical presentation in light of the patient’s com-munication ability,
cognitive level, associated disabilities (e.g., sensory), life experiences,
environmental factors and cultural background. One should differentiate between
be-haviors appropriate for an earlier age and those that are patho-logical in
any age (e.g., true hallucinations). Not all disruptive behaviors are an
expression of a mental disorder: for example, an overworked staff might promote
aggressive acting out by attending to the patients only when they become
aggressive. However, one should not simply explain all such behaviors as
attention-seeking behaviors. Conversely, persons who do not manifest disruptive
behaviors might have a mental disorder, for example, a depressed individual who
is considered behav-ing well because he is very quiet.
· Obtain,
if needed, evaluations and consultations with other disciplines, for example,
language pathologists, psychologists and neurologists.
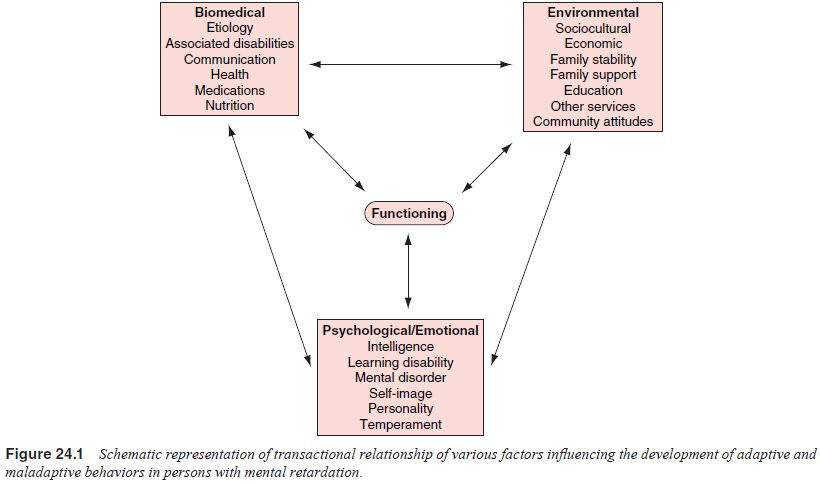
· Assess
and understand the dynamic, ongoing transactional relationships among the
various factors contributing to the person’s development (see Figure 24.1).
·
Try to make a formal Axis I and/or Axis II DSM-IV
diagnosis (besides mental retardation) whenever clinically justified. The
diagnostic criteria can usually be adapted to the patient’s de-velopmental
level, just as one does with child patients). How-ever, diagnosis does not mean
listing the disorder’s code and name only. To be constructive, the diagnostic
statement should include description of strengths, impairments, and need for
supports and services in each discrete domain of the individu- al’s
functioning, as well as in the environment (community and family). It should
not merely copy the diagnostic criteria but describe how they are satisfied in
the particular case by history and clinical observation, as well as why other
diag-noses in the differential are ruled out.
Aggression
“Aggression” to people or property (destructiveness)
is one of the most frequent reasons (if not the most frequent) for refer-ring
persons with mental retardation to a psychiatrist. On closer investigation, the
actual behavior ranges from occasional swearing (verbal aggression) to serious
violence (Harris, 1995). Whether a particular behavior is called aggression
(except for clear physical aggression) depends on the caregiver’s perception.
Thus, in ob-taining the history it is necessary to obtain a concrete
description of the behavior in question, preferably from several informants.
Prolonged direct observation of the patient may be necessary to resolve unclear
cases. There is no single entity called aggression in this population that
would have one explanation. It would be a mistake to talk about a single
treatment for aggression (except for symptomatic emergency measures).
Psychiatrists are often asked how they treat aggression in persons with mental
retardation. The answer is, of course, that it is done in the same manner as in
persons without mental retardation: an accurate diagnostic as-sessment comes
first. Different factors must be considered in as-sessing the cause of
aggressive behavior (Harris, 1995). It might be associated with a defined
mental disorder, for example, ag-gression following a command hallucination,
paranoid delusion, anxiety, borderline or antisocial personality, or
depression. The factor of learning will reinforce aggressive behavior if it
brings a desired response by the caregivers. A pathological brain condi-tion, such
as rage attacks after brain trauma or associated with temporo-limbic seizure
disorder, may also lead to aggression. Often, several causative factors are
involved, all of which require evaluation and intervention.
The DSM-IV-TR has a category of intermittent
explosive disorder that can be used provided that another mental disorder has
been ruled out as the cause of the aggressive behavior.
Related Topics