Chapter: Clinical Dermatology: Infestations
Lice infestations (pediculosis)
Lice
infestations (pediculosis)
Lice
are flattened wingless insects that suck blood. Their eggs, attached to hairs
or clothing, are known as nits. The main feature of all lice infestations is
severe itching, followed by scratching and secondary infection.
Two
species are obligate parasites in humans: Pediculus humanus (with
its two varieties
P. humanus capitis, the head louse, and P.
humanus corporis, thebody louse) and Phthirus pubis
(the pubic louse).
Head lice
Cause
Head
lice are still common, affecting up to 10% of children even in the smartest
schools. The head louse itself measures some 3–4 mm in length and is greyish,
and often rather hard to find. However, its egg cases (nits) can be seen easily
enough, firmly stuck to the hair shafts. Spread from person to person is
achieved by head-to-head contact, and perhaps by shared combs or hats.
Presentation and course
The
main symptom is itching, at first around the sides and back of the scalp and
then more generally over it. Scratching and secondary infection soon follow
and, in heavy infestations, the hair becomes matted and smelly. Draining lymph
nodes often enlarge.
Complications
Secondary
bacterial infection may be severe enough to make the child listless and
feverish.
Differential diagnosis
All
patients with recurrent impetigo or crusted eczema on their scalps should be
carefully examined for the presence of nits.
Investigations
None
are usually required.
Treatment
Malathion,
carbaryl and permethrin preparations (Formulary 1) are probably the treatments
of choice now. They kill lice and eggs effectively; malathion has the extra
value of sticking to the hair and so protecting against reinfection for 6
weeks. The policy whereby public health authorities rotate their use, with the
aim of lessening the risk of resistant strains emerging, has fallen out of
favour now.
Lotions
should remain on the scalp for at least 12 h, and are more effective than
shampoos. The applica-tion should be repeated after 1 week so that any lice
that survive the first application and hatch out in that interval can be
killed. Other members of the family and school mates should be checked. A
toothcomb helps to remove nits but occasionally matting is so severe that the
hair has to be clipped short. A systemic antibiotic may be needed to deal with
severe secondary infection. Some recommend, as an alternative to the treatments
mentioned above, that the hair should be combed repeatedly and meticulously
with a special ‘detection comb’abut the efficacy of this method has still to be
established. However, a head louse repel-lent, containing 2% piperonal, is
available over the counter and may be worth a trial for those who are
repeatedly reinfested. Systemic ivermectin therapy is reserved for infestations
resisting the treatments listed above.
Body lice
Cause
Body
louse infestations are now uncommon except in the unhygienic and socially
deprived. Morpholo-gically the body louse looks just like the head louse, but
lays its eggs in the seams of clothing in contact with the skin. Transmission
is via infested bedding or clothing.
Presentation and course
Self-neglect
is usually obvious; against this back-ground there is severe and widespread
itching, espe-cially on the trunk. The bites themselves are soon obscured by
excoriations and crusts of dried blood or serum. In chronic untreated cases
(‘vagabond’s disease’) the skin becomes generally thickened,eczematized and
pigmented; lymphadenopathy is common.
Differential diagnosis
In
scabies, characteristic burrows are seen. Other causes of chronic itchy
erythroderma include eczema and lymphomas, but these are ruled out by the
finding of lice and nits.
Investigations
Clothing
should be examined for the presence of eggs in the inner seams.
Treatment
First
and foremost treat the infested clothing and bedding. Lice and their eggs can
be killed by high tem-perature laundering, by dry cleaning and by
tumble-drying. Less competent patients will need help here. Once this has been
achieved, 5% permethrin cream rinse or 1% lindane lotion (USA only) (Formulary
1) may be used on the patient’s skin.
Pubic lice
Cause
Pubic
lice (crabs) are broader than scalp and body lice, and their second and third
pairs of legs are well adapted to cling on to hair. They are usually spread by
sexual contact, and most commonly infest young adults.
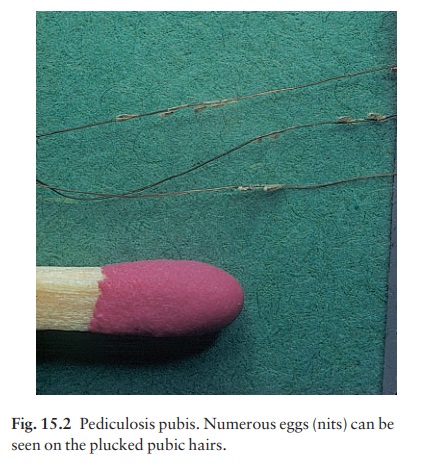
Presentation
Severe
itching in the pubic area is followed by eczema-tization and secondary
infection. Among the excoria-tions will be seen small blue-grey macules of
altered blood at the site of bites. The shiny translucent nits are less obvious
than those of head lice (Fig. 15.2). Pubic lice spread most extensively in
hairy males and may even affect the eyelashes.
Differential diagnosis
Eczema of the pubic area gives similar symptoms but lice and nits are not seen.
Investigations
The
possibility of coexisting sexually transmitted dis-eases should be kept in
mind.
Treatment
Carbaryl,
permethrin and malathion are all effective treatments. Aqueous solutions are less
irritant than alcoholic ones. They should be applied for 12 h or overnight to
all parts of the trunk, including the peri-anal area and to the limbs, and not
just to the pubic area. Treatment should be repeated after 1 week, and infected
sexual partners should also be treated. Shaving the area is not necessary.
Infestation
of the eyelashes is particularly hard to treat, as this area is so sensitive
that the mechanical removal of lice and eggs can be painful. Applying a thick
layer of petrolatum twice a day for 2 weeks has been recommended. Aqueous
malathion is effective for eyelash infestations but does not have a product
licence for this purpose.
Related Topics