Chapter: Clinical Cases in Anesthesia : Gastroschisis and Omphalocele
How is this neonate managed preoperatively?
How is this neonate managed preoperatively?
Immediately after birth, the exposed
intra-abdominal contents should be wrapped in a sterile dressing which is then
kept warm and moist. Plastic coverings may also help to decrease heat and fluid
loss. It is important to monitor and maintain temperature preoperatively.
Preoperative preparation should include placement of an intravenous catheter
for fluid replacement. An arterial catheter may be placed for frequent
laboratory analysis, including measure-ments of blood glucose.
Infants are more susceptible to dehydration
because of their increased metabolic rate and water losses. Insensible fluid
losses are greater in infants because of their greater surface area/weight
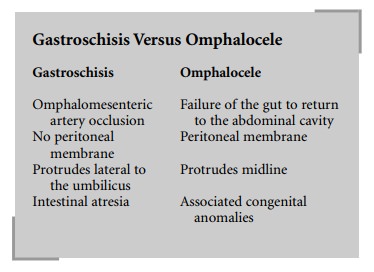
ratio and thinner skin. In addition, gastroschisis, omphalocele, pyloric
stenosis, intussuscep-tion, and many other processes can cause significant
elec-trolyte and fluid imbalances.
Assessment of volume status involves many
variables: moistness of mucous membranes, skin turgor, weight, mean arterial
pressure, capillary perfusion time, urine output, peripheral pulse quality, and
heart rate. Significant fluid deficits and electrolyte imbalances should be
cor-rected preoperatively. Initially a balanced salt solution should be used to
increase blood volume and replace third-space losses. Fluid replacement should
also include main-tenance fluids, with or without glucose, depending on blood
glucose analysis. Excess glucose can be detrimental since the neonatal kidney
can spill glucose easily, resulting in an osmotic diuresis. As replacement
occurs, multiple parameters need to be monitored to assess hydration sta-tus,
such as vital signs, urine output, clinical examination, and laboratory values.
Maintaining temperature is critical during the
peri-operative period since hypothermia is a potential risk. Hypothermia causes
an increase in the metabolic rate with increased oxygen consumption resulting
in hypoxemia, acidosis, and possibly apnea. The neonate attempts to main-tain
body temperature through nonshivering thermogenesis. This is accomplished by
the metabolism of brown fat, which is more abundant in newborns than in adults.
Brown fat metabolism is stimulated by norepinephrine released through
sympathetic innervation in an attempt to maintain core temperature at a great
metabolic cost.
The intestines are susceptible to both
morphologic and functional compromise, especially in gastroschisis due to the
lack of a protective peritoneal membrane and possible pre-existing fetal
peritonitis. Bowel atresia is seen in about 10% of cases. Care should be taken
to avoid traumatizing the exposed bowel and to avoid incarceration at the site
of extrusion.
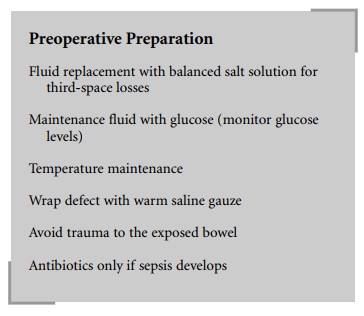
Although sepsis may occur, there is no
indication for the administration of prophylactic antibiotics.
The neonate should be examined for other
associated congenital anomalies, especially those involving the cardio-vascular
and pulmonary system, which may affect mor-bidity and mortality. Omphalocele
can be a part of the Beckwith-Wiedemann syndrome, which also includes macroglossia,
gigantism, organomegaly, and symptomatic hypoglycemia. Neonates with
Beckwith-Wiedemann syn-drome are known to have a difficult airway due to the
macroglossia.
Related Topics