Chapter: Clinical Cases in Anesthesia : Gastroschisis and Omphalocele
How is the operating room prepared for this newborn?
How is the operating room prepared for this newborn?
Before any pediatric patient is brought to the
operating room, appropriately sized equipment must be prepared for both
anesthesia and surgery. Mnemonics may be used to aid in making sure that all
critical equipment is available. This has added importance when preparing for a
neonate, infant, or child because they will require equipment that is not
normally stocked in the operating room, except in a pediatric hospital. A
useful mnemonic is MADIMS, which stands for Machine,
Airway, Drugs, Intravenous, Monitors, and Suction.
Machine
Preparing the machine includes following the
standard US Food and Drug Administration (FDA) Anesthesia Apparatus Checkout
Recommendations, 1993. It is necessary to choose a breathing circuit, either a
Mapleson D or a pediatric circle system. The pediatric circle system differs
from the adult in that it has hoses that are of lower volume and compliance,
which may allow for more constant tidal volumes. Also, heated humidified
circuits are available, which can conserve heat and decrease evaporative
losses. Some older anesthesia machines have separate pediatric bellows, which
may increase the accuracy of delivering very small tidal volumes. Also, the
ability to add air to the gas mixture should be assured. This may be necessary
for the premature infant, when nitrous oxide cannot be used, in order to avoid
high arterial oxygen partial pressures and limit the risk of retinopathy of
prematurity.
Airway
Airway equipment is available in all sizes and
styles and the anesthesiologist should use the equipment with which he or she
is most familiar. The key is to have the appropri-ate sizes available. This
includes masks, oral airways, laryn-geal mask airways, endotracheal tubes
(ETT), and laryngoscope blades. The best way to be prepared is to have the size
that you think you will need and also one size above and below that size. Oral
airways are available from size 000 (very small premature neonates) to 9 (large
adult). Nasal airways are rarely used in young children due to the risk of
adenoidal hemorrhage and the small lumen of the nares. A straight laryngoscope
blade (Miller 0 for preterm infants, Miller 0–1 for full-term infants) is often
used in neonates and infants.
Uncuffed ETTs have historically been used in
infants and children under age 7 years, but a new trend is developing for the
use of cuffed tubes in younger age groups. There are many factors to consider
when making this decision. In a young child, the narrowest portion of the
airway is at the cricoid ring. An ETT should be selected that is neither too
small to adequately ventilate the patient nor too large to cause damage to the
subglottic area. An important factor, whether the ETT is cuffed or uncuffed, is
to have an appro-priate air leak, which is <30 cm H2O in most
cases. A general rule for choosing uncuffed tubes in children ages 2 years and
above is: [Age + 16]/4.
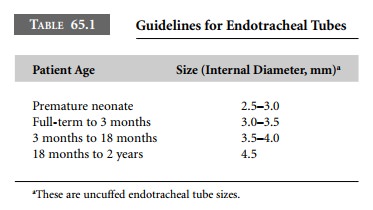
If a cuffed ETT is chosen, it should be a
half-size smaller. Most full-term neonates will have an appropriate leak with a
3.0 uncuffed ETT, and by a few months of age a 3.5 uncuffed ETT can be used
(Table 65.1). After placing the correct size ETT, it is critical to secure it
well since even the slightest movement of the ETT in a neonate could result in
a mainstem intubation or extubation. If a cuffed ETT is used, the cuff should
be inflated only if the air leak is less than that needed to provide adequate
positive pres-sure ventilation. A leak at <30 cm H2O should be
present. During the course of the case, the air leak should be checked since
the use of nitrous oxide as part of the anesthetic may increase the volume in
the cuff. If lung compliance changes during surgery, it may be necessary to add
air to the cuff to increase the air leak pressure and improve ventilation.
Drugs
Drugs refer to both the anesthetic and
non-anesthetic medications that should be drawn up and immediately available
during the anesthetic. These include induction agents, muscle relaxants, and
opioids, as well as emergency medications such as atropine and epinephrine. The
appro-priate dose of these drugs should be determined in advance, based on the
weight of the patient, and drawn up in an appropriately sized syringe.
Intravenous
Intravenous fluid and supplies for placing an
intravenous line should be available in the operating room. A buretrol should
be a part of the set and no more than 10 mL/kg of fluid should be in the
buretrol at any time to prevent fluid overload if it accidentally ran in
quickly. All air bubbles should be removed from the intravenous tubing because
there is a high incidence of patent foramen ovale in neonates.
Monitors
Monitors should include all those set forth by
the American Society of Anesthesiologists (ASA) in their Standards for Basic
Intraoperative Monitoring, last amended in October 1998. All other monitors
will be based on the clinical condition of the patient and the type of surgery
planned.
Suction
Suction should be immediately available and
within easy reach of the anesthesiologist. A Yankauer is the best for large
volumes because of its large holes, but in small infants it may be necessary to
use smaller suction catheters.
Methods for maintaining normothermia in the
neonate should also be made available. This is best accomplished with a
forced-air warming blanket and warming of the operating room.
Related Topics