Chapter: Clinical Cases in Anesthesia : Preeclampsia
How is preeclampsia prevented from degenerating into eclampsia?
How is
preeclampsia prevented from degenerating into eclampsia?
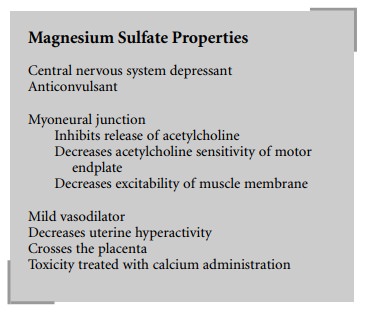
Magnesium sulfate (MgSO4), a central
nervous system depressant and anticonvulsant, is the first-line drug in the
United States for the prevention of eclampsia. One of the many sites of action
of MgSO4 is at the myoneural junction.
The decrease in hyperreflexia seen with the
administration of MgSO4 is secondary to the inhibition of
acetylcholine release at the neuromuscular junction, decreased sensitivity of
the motor endplate to acetylcholine, and the decreased excitability of the
muscle membrane. MgSO4 is also a mild vasodilator and decreases
uterine hyperactivity, which results in an increase in uterine blood flow. It
also causes vasodilation at the renal and liver beds thus improving their
function.
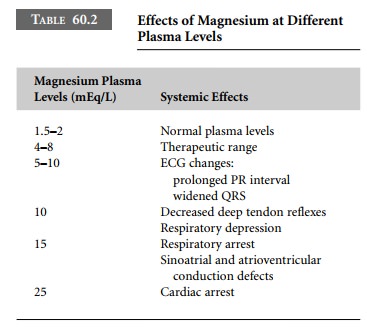
Therapeutic levels of magnesium are between 4
and 8 mEq/L. Above this level, magnesium has both maternal and neonatal
side-effects. Magnesium can lead to elec-trocardiographic changes and
ultimately cardiac and respiratory arrest. These severe side-effects, however,
do not occur until after the loss of deep tendon reflexes (Table 60.2).
Therefore, by monitoring serum magnesium levels and deep tendon reflexes
catastrophic side-effects may be avoided. Magnesium, because of its actions at
the neuromuscular junction, increases the sensitivity of the mother to both
depolarizing and nondepolarizing muscle relaxants.
Since magnesium crosses the placenta, the
neonate can also exhibit signs of magnesium toxicity. Signs of magne-sium
toxicity in the newborn include respiratory depression, apnea, and decreased
muscle tone. Magnesium toxicity in the newborn and the mother can be reversed
with the administration of calcium.
MgSO4 is administered intravenously
with a loading dose of 2–4 grams over 15 minutes, followed by an infusion of
1–3 grams per hour. MgSO4 is primarily excreted by the kidneys.
Therefore, renal function must be carefully moni-tored and the magnesium dose
decreased accordingly in the face of renal insufficiency.
Related Topics