Chapter: Clinical Cases in Anesthesia : Preeclampsia
Explain the management of preeclampsia-related hypertension
Explain the management of preeclampsia-related hypertension.
Control of hypertension in the parturient with
preeclampsia is imperative since acute elevations of blood pressure can lead to
cerebral hemorrhage, the leading cause of mortality. The patient’s blood
pressure should be neither acutely decreased nor decreased to levels considered
nor-mal for other parturients since a low blood pressure could compromise
uteroplacental blood flow. Although MgSO4 causes vasodilation, it does
not treat hypertension adequately and an alternative antihypertensive drug is
usually needed. Also, as in any patient with hypertension, responses to both
antihypertensive and pressor agents are exaggerated. Therefore, reduced doses
of these agents should be used initially and the response noted prior to
increasing the dose.
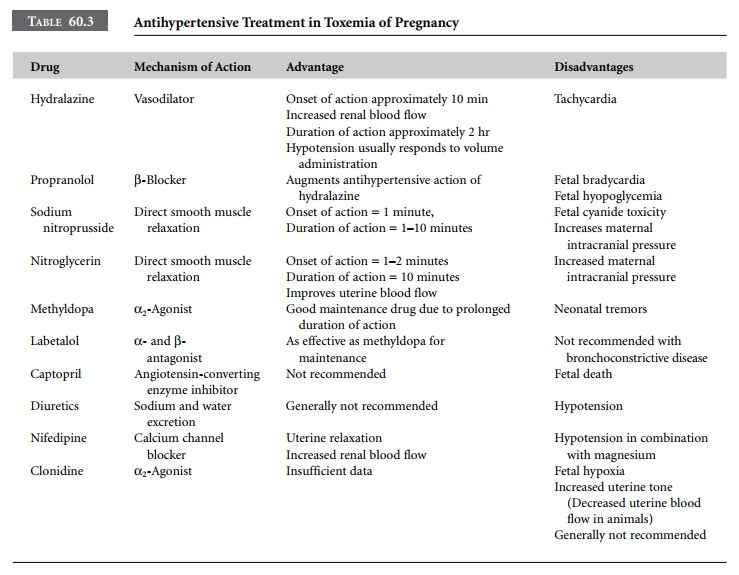
The most frequently used antihypertensive agent
is hydralazine, which not only decreases blood pressure but also increases
renal and uteroplacental blood flow. The tachycardia that occurs with the use
of hydralazine can be treated with propranolol. Hydralazine is not the agent of
choice in the acute situation since it takes 10–15 minutes before an effect is
seen.
Nitroprusside, a potent arterial vasodilator,
is often used when immediate control of blood pressure is required. It is
administered by infusion making it easy to titrate to effect. Nitroprusside,
however, crosses the placenta and cyanide toxicity has been described in the
neonate after prolonged infusion in the mother. Trimethaphan, a ganglionic
blocker, has also been used with good success in the emergent situation.
Nitroglycerin, a venous dilator, is useful when
tight con-trol of blood pressure is required for prolonged periods.
Nitroglycerin is not as potent as nitroprusside but is easy to titrate and has
minimal effect on the fetus.
Propranolol, diazoxide, methyldopa, and
captopril are generally not used in the patient with preeclampsia because of
their adverse side-effects (Table 60.3).
Related Topics