Chapter: Clinical Anesthesiology: Anesthetic Management: Geriatric Anesthesia
Geriatric Anesthesia
Geriatric Anesthesia
By the year 2040, persons aged 65 years or
older are expected to comprise 24% of the population and account for 50% of
health care expenditures. In Europe, persons aged 65 years or older are
expected to comprise 30% of the population within the next 40 years. Of these
individuals, many will require surgery. The elderly patient typically presents
for surgery with multiple chronic medical conditions,
in addition to the acute surgical illness. Age is not a contraindication
to anesthesia and surgery; however, perioperative morbidity and mortality are
greater in elderly than younger surgical patients.
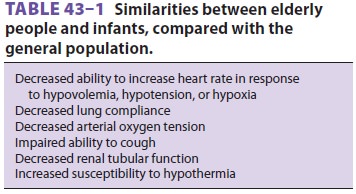
As with pediatric patients, optimal
anesthetic management of geriatric patients depends upon an understanding of
the normal changes in physi-ology, anatomy, and response to pharmacological
agents that accompany aging. In fact, there are many similarities between
elderly and pediatric patients (Table 43–1).
Individual genetic polymorphisms and lifestyle choices can modulate the
inflammatory response, which contributes to the development of many systemic
diseases. Consequently, chronologic age may not fully reflect an individual
patient’s true physical condition. The relatively high frequency of serious
physiological abnormalities in elderly patients demands a particularly careful
preoperative evaluation.
Elderly patients are frequently treated with β-blockers.
β-Blockers should be continued
peri-operatively, if patients are taking such medications chronically, to avoid
the effects of β-blocker with-drawal. A
careful review of patients’ often exten-sive medication lists can reveal the
routine use of oral hypoglycemic agents, angiotensin-converting enzyme
inhibitors or angiotensin receptor block-ers, antiplatelet agents, statins, and
anticoagulants. Because elderly patients frequently take multiple drugs for
multiple conditions, they often benefit from an evaluation before the day of
surgery, even when scheduled for outpatient surgery. Preoperative laboratory
studies should be guided by patient con-dition and history. Patients who have
cardiac stents requiring antiplatelet therapy present particularly vexing
problems. Their management should be closely coordinated between the surgeon,
cardi-ologist, and anesthesiologist. At no time should the anesthesia staff
discontinue antiplatelet therapy without discussing the plan with the patient’s
pri-mary physicians.
Related Topics