Chapter: Medical Microbiology: An Introduction to Infectious Diseases: Enteric Infections and Food Poisoning
General Diagnostic Approaches - Enteric Infections and Food Poisoning
GENERAL DIAGNOSTIC APPROACHES
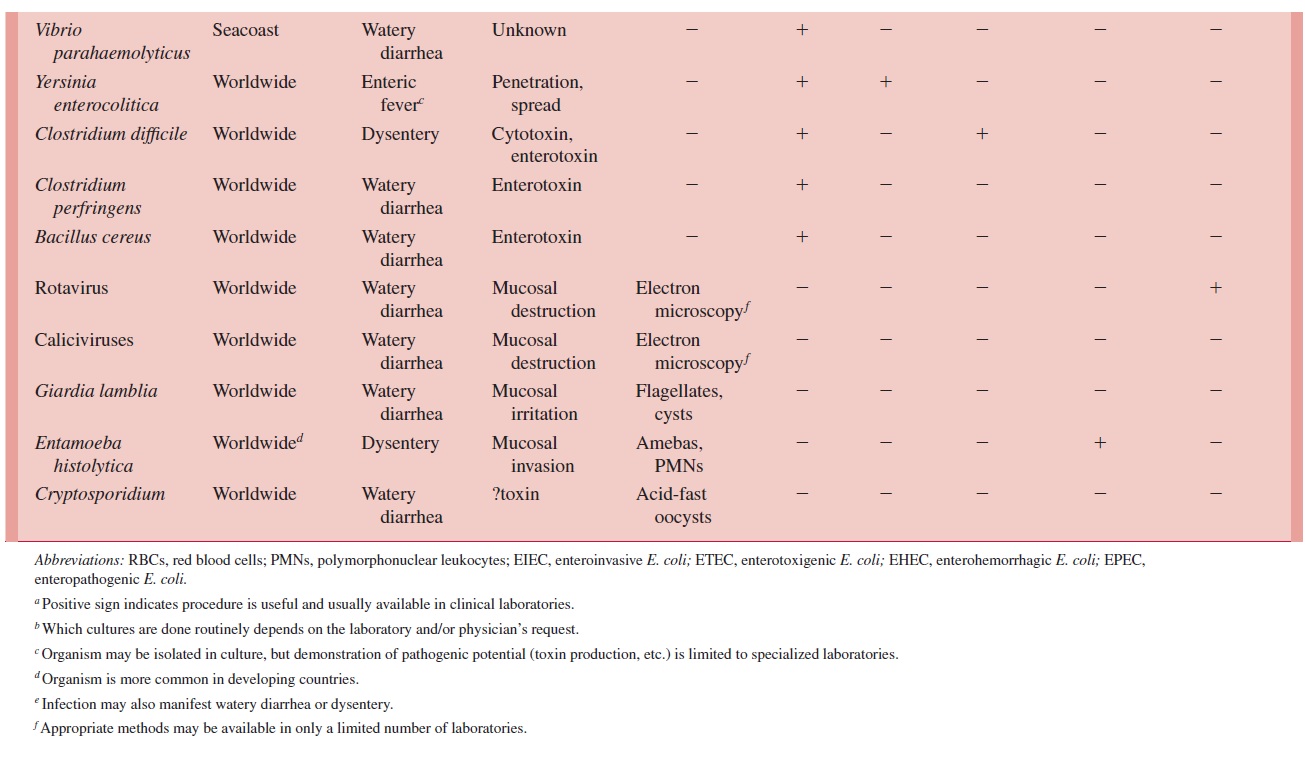
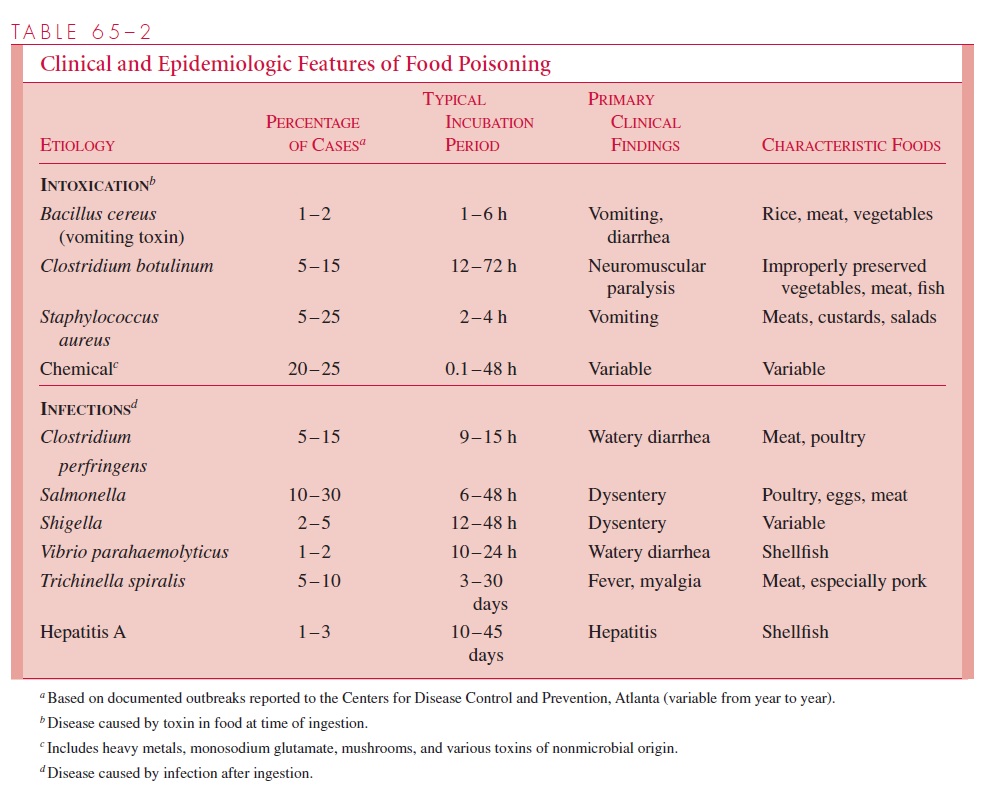
Laboratory diagnostic procedures (summarized in Table 65 – 1) include microscopic ex-amination, culture, toxin detection, and serologic procedures. The relative value of each is different for the various etiologies. The diagnostic approach therefore requires that the physician assess the clinical and epidemiologic features of the case, decide which organ-isms are potential causes, and provide this assessment to the laboratory so that appropri-ate procedures will be used.
Microscopic Examination
Microscopic examination is of value in the assessment of bacterial infections when they are positive. The presence of polymorphonuclear leukocytes or blood in the stool corre-lates with organisms that produce disease by invasion, but false-negative results are com-mon. The leukocytes may be seen in unstained or methylene blue – stained wet mount preparations; the absence of fecal leukocytes, however, does not exclude invasive diar-rhea. The observation and morphologic characterization of amebas and flagellates on wet or stained preparations are the primary means by which amebic (Entamoeba histolytica) and flagellate (Giardia lamblia) infections are diagnosed. Rotaviruses and other viruses of diarrhea cannot be grown in cell culture but can be detected by electron microscopy.
Culture
Isolation of the etiologic agent is the primary means by which bacterial enteric infection is diagnosed. In enteric fever the organism is typically present in the blood in the early stages of disease. Blood cultures are, however, usually negative in watery diarrhea and dysenteric infections, and stool culture must be relied upon for diagnosis. Fortunately, several good selective media have been developed for both direct plating and enrichment culture, which allow isolation of the infecting organism in the presence of a predominant normal flora. Selective media are then used for the various enteric pathogens . Media routinely used may vary between clinical laboratories but should include those appropriate for Salmonella, Shigella, and Campylobacter jejuni. Diarrhea caused byE. coli is a special problem, because the methods that define the enterotoxigenic, invasive,or other pathogenic mechanisms are not yet practical for clinical laboratories.
Toxin Assay
The B cytotoxins of C. difficile can be detected by its cytopathic effect in a cell culture system. In most clinical cases, enough toxin is present for direct detection in a stool spec-imen. This assay is currently available only in reference laboratories. Methods that detect the C. difficile A and B toxins by latex agglutination are now in common use. The cost-benefit of various combinations of toxin detection methods is still controversial.
Antigen and Antibody Detection
At present, antibody detection is useful in the diagnosis of amebic dysentery caused by E.histolytica and of typhoid fever. Both are considered ancillary to the primary diagnostic tests, which involve specific detection of the organism by microscopic and cultural meth- ods. Reagents are commercially available for the detection of rotavirus antigen in stool by latex agglutination or enzyme immunoassay. These methods have a sensitivity roughly comparable to that of electron microscopy. Serologic methods have been described formany other causes of gastrointestinal infection but are not generally used because of lackof sensitivity, specificity, or availability of reagents.
Related Topics