Chapter: Clinical Cases in Anesthesia : The Difficult Airway
Discuss the risk factors for difficult intubation
Discuss the risk factors for difficult intubation.
Sniffing Position
The presence or absence of airway pathology
does not influence the definition of difficult tracheal intubation. It occurs
when multiple attempts at intubation are required. Traditional laryngoscopy is
performed in order to visualize the laryngeal opening. The laryngoscopist is
positioned outside the airway, above the patient’s head. To see through the
airway, light must travel from the glottic opening to the laryngoscopist’s eye.
This technique requires an uninter-rupted linear path between the larynx and
laryngoscopist because light generally travels in a straight line. Most
manipulations performed attempt to satisfy this criterion.
The airway contains three visual axes. They are
the long axes of the mouth, oropharynx, and larynx. In the neutral position,
these axes form acute and obtuse angles with one another. Light cannot bend
around these angles under normal circumstances. In order to bring all three
axes into better alignment, Magill suggested “Sniffing the morning air
position.” True sniffing position requires both cervical flexion and
atlanto-occipital extension. Cervical flexion approximates the pharyngeal and
laryngeal axes. Atlanto-occipital extension brings the oral axis into better alignment
with the other two. Normal atlanto-occipital extension measures 35°. With
optimal alignment of the airway’s visual axes, it becomes possible to look
through the airway into the laryngeal opening. Reduced atlanto-occipital gap or
prominent C1 spinous processes impairs laryngoscopy if vigorous attempts at
extension are performed because the larynx is forced anteriorly causing the
trachea to bow.
Inability to assume the sniffing position is a
predictor of difficult intubation. Examples of problems that prevent sniffing
position include cervical vertebral arthritis, cervical ankylosing spondylitis,
unstable cervical fractures, pro-truding cervical discs, atlanto-axial
subluxation, cervical fusions, cervical collars, and halo frames. Morbidly
obese patients sometimes have posterior neck fat pads that prevent
atlanto-occipital extension.
The ability to achieve the sniffing position is
easily tested: simply have the patient flex the lower cervical verte-brae and
extend at the atlanto-occipital joint. Pain, tingling, numbness, or inability
to achieve these maneuvers predicts difficult intubation.
The benefits of the sniffing position have been
dogma for over 70 years. More recently, Adnet et al. (2001) and Chou and Wu
(2001) have independently questioned its utility.
Mouth Opening
Mouth opening is important because it
determines the available space for placing and manipulating the laryngo-scope
and tracheal tube. A small mouth opening may not accommodate either one. Mouth
opening also facilitates visualization of the uppermost part of the airway.
Mouth opening relies on the temporomandibular joint (TMJ), which works in two
ways. It has both a hinge-like move-ment and a gliding motion. The gliding
motion is known as translation. Its hinge-like movement allows the mandible to
pivot on the maxilla. The more the mandible swings away from the maxilla, the
bigger the mouth opening. The adequacy of mouth opening is assessed by
measuring the inter-incisor distance. An inter-incisor distance of 3 cm
provides sufficient space for intubation, in the absence of other complicating
factors. This corresponds approximately to the width of 2 finger breadths. The
2 finger breadth test is performed by placing the examiner’s 2nd and 3rd digits
between the patient’s central incisors. If they fit, there should be adequate
room to perform laryngoscopy. If they do not fit, then laryngoscopy may be
difficult. Factors that interfere with mouth opening include masseter muscle
spasm, TMJ dysfunction, and various integumentary ailments, such as burn scar
contractures and progressive systemic sclerosis. Masseter muscle spasm may be
relieved by induction of anesthesia and administration of muscle relaxants. TMJ
mechanical problems remain unaltered by medications. Some patients demonstrate adequate
mouth opening when awake, but not after anesthetic induction. The problem can
oftentimes be relieved by pulling the mandible forward. A mouth opening that
was sufficient for a previous anes-thetic may not be after temporal
neurosurgical procedures.
Dentition
Instrumentation of the airway places teeth at
risk for damage. Multiple problems result from dental injury. Teeth may be
dislodged or broken. Such teeth cannot be used for chewing, may be painful, and
will be costly to repair. Beyond these issues, broken teeth can fall into the
trachea, migrate to the lung, and predispose to abscesses. Poor dentition is at
risk for damage as the mouth is opened and as the laryngoscope blade is
introduced. Teeth that can be extracted easily with digital pressure should
probably be removed. During laryn-goscopy in the presence of poor dentition,
extra efforts are made to avoid placing pressure on the maxillary incisors. In
doing so, the laryngoscope is manipulated into a less than ideal position
resulting in poor visualization of the glottis.
Prominent maxillary incisors complicate
laryngoscopy in another way. They protrude into the mouth and block the line of
sight to the larynx. In order to overcome this problem, laryngoscopists must
adjust their line of sight. To accomplish this, the laryngoscopist’s eye is
brought to a new position that is higher than the original one. The
laryngoscopist then looks tangentially over the protruding maxillary incisor.
This creates two new points in the adjusted line of sight and, thus, a new
straight line of sight. The new line of sight brings the laryngoscopist’s view
to a more posterior laryngopharyngeal position. This results in a view that is
posterior to the larynx. Consequently, the larynx is not visualized and a
difficult laryngoscopy is produced. In much the same way, edentulous patients
tend to be easy intubations, because the laryngoscopist can adjust the line of
sight to a more advantageous angle.
Tongue
The tongue occupies space in the mouth and
oropharynx.
The base of the tongue resides close to the
glottic aperture. During traditional direct laryngoscopy, the base of the
tongue falls posteriorly obstructing the line of sight into the glottis.
Visualizing the larynx requires displacing the base of the tongue anteriorly,
so that the line of sight to the glottis is restored. The tongue is frequently
displaced with hand-held rigid laryngoscope, to which Macintosh and Miller
blades are the most commonly attached. Laryngoscopes push the tongue anteriorly
and, in so doing, move it from a posterior obstructing position to a new
anterior non-obstructing position within the mandibular space. The mandibular
space is that area between the two rami of the mandible. Even with the tongue
maximally displaced into the mandibular space, visualization of the larynx is
sometimes inadequate.
Usually, a normal-size tongue fits easily into
a normal-size mandibular space, whereas a large tongue would fit poorly. After
filling the space, a large tongue still occupies some of the oropharyngeal
airway causing obstruction. For this reason, a large tongue (macroglossia) is a
predictor of a difficult intubation. Similarly, a normal-size tongue fits
poorly into a small mandibular space. It too occupies some of the oropharyngeal
airway, thereby obstructing the line of sight. Consequently, a small mandible
(micrognathia) is predictor of a difficult intubation. In essence, a tongue
that is large compared with the size of the mouth, orophar-ynx, and mandible
takes up excessive space in the orophar-ynx and interferes with visualization.
The base of the tongue resides so close to the
larynx that inability to adequately displace it anteriorly creates another
problem. As the base of the tongue hangs down over the larynx, the glottis is
hidden from view. The glottic aperture is then anatomically anterior to the
base of the tongue, hence the term “anterior larynx.” Under such circum-stances
the larynx is anterior to the base of the tongue and cannot be seen because the
tongue hides it. Glottic and supraglottic masses that force the base of the
tongue poste-riorly can create difficult intubations as well. Some of the
masses that may be encountered include lingual tonsils, epiglottic cysts, and
thyroglossal duct cysts.
After filling the mandibular space with the
tongue, additional pressure on the laryngoscope blade lifts the mandible
anteriorly. In this setting, mandibular displace-ment is dependent upon the
TMJ. In addition to its hinge-like motion, the TMJ also works in a gliding
(translational) movement. It is the gliding motion that allows the mandible to
slide anteriorly across the maxilla. If the joint does not translate, the
mandible cannot be displaced anteriorly and the tongue cannot be moved out of
the line of sight.
Recognizing the implications of tongue size to
successful laryngoscopy, Mallampati et al. in 1985 and Samsoon and Young in
1987 devised classification systems to predict difficult laryngoscopy,
utilizing this concept. A difficult laryngoscopy occurs when it is not possible
to visualize any portion of the vocal cords. Mallampati and Samsoon reasoned
that a large tongue could be identified upon visual inspection of the open
mouth. Both classification systems relate the size of tongue to the
oropharyngeal structures identified. A normal-size tongue allows for
visu-alization of certain oropharyngeal structures. As the tongue size
increases, some structures become hidden from view. Consequently, both
investigators proposed systems that reason backwards from this premise.
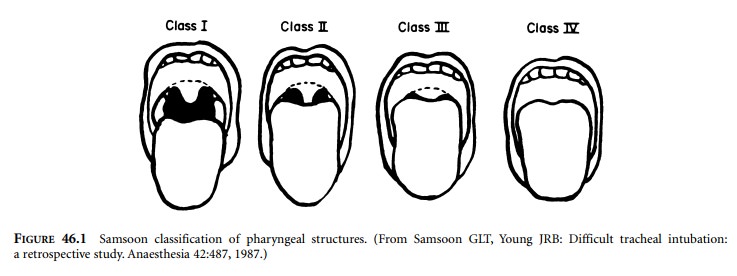
Application of the Mallampati and/or Samsoon
classifi-cation system(s) is easy and painless. The patient is seated in the
neutral position. The mouth is opened as wide as it can and the tongue is
protruded as far as possible. Phonation is discouraged because it raises the
soft palate and allows for visualization of additional structures. The observer
looks for specified anatomic landmarks. They are the fauces, pillars, uvula,
and soft palate. The Mallampati classification system utilizes three groups and
the Samsoon classification system employs four groups (Figure 46.1). Both
systems suggest that as the tongue size increases, fewer structures are
visualized and laryngoscopy becomes more difficult. Mallampati scores tend to
be higher in preg-nant versus nonpregnant patients.
Just as the size of tongue can be estimated, so
too can the size of the mandible. This is accomplished by asking the patient to
extend their head at the atlanto-occipital joint and identifying the mandibular
mentum and thyroid carti-lage. The Adam’s apple (thyroid notch) is the most
superfi-cial structure in the neck and serves as a good landmark for the
thyroid cartilage. The vocal cords lie just caudad to the thyroid notch. The
distance between the thyroid cartilage and mentum (thyromental distance) is
measured in one of three ways. The measurement can be made with a set of
spacers, a small pocket ruler, or with the observer’s fingers. The normal
thyromental distance is 6.5 cm. A thyromental distance of greater than 6 cm is
predictive of an easy intubation. A thyromental distance of 6 cm or less is
suggestive of a difficult intubation. Oftentimes, rulers are not present at the
bedside. In the absence of a ruler, practitioners can judge the thyromental
distance with their fingers. By knowing the width of one’s middle three
fingers, which frequently approximates 6 cm, the thyromental distance can be
compared with the fingers’ span. In this way, clini-cally relevant
approximations can be taken into account when examining patients for the
purpose of predicting difficult intubation. The usefulness of predicting
diffi-cult intubation based on thyromental distance has been challenged. Data
extracted from Rocke et al.’s 1992 paper and El-Ganzouri’s 1996 paper show that
thyromental distance (receding mandible) offers a 7% or less probabil-ity of
predicting difficult intubation. Chou in 1993 and Brodsky in 2002 describe
patients whose thyromental dis-tances were well in excess of 6.5 cm and who
were difficult intubations.
Similar measurements and predictions have been
made utilizing the hyoid bone and mandible, as well as the sternum and mentum.
Chou and Wu (2001) suggest that a long mandibulohyoid distance predicts a large
hypopharyngeal tongue, which hides the glottis during laryngoscopy and thereby
produces a difficult intubation. They reason that the tongue is hinged to the
hyoid bone, so that a long hyomandibular length represents a caudad-lying
tongue. With the base of the tongue positioned farther inferiorly, it occupies
more space in the oropharyngeal airway. Consequently, it obstructs the
laryngoscopist’s line of sight. The hyoid bone is more difficult to feel than
the thyroid cartilage and is oftentimes impossible to locate. The sternum and
mentum are generally easy to find, but the sternomental distance has not been substantiated
as a good predictor of difficult intubation by other investigators.
The ability to translate the TMJ is easily
assessed prior to induction. The patient is asked to place the mandibular
inci-sors (bottom teeth) in front of the maxillary incisors (upper teeth).
Inability to perform this simple task is usually from one of two sources.
First, the TMJ may not glide, thereby predicting a difficult intubation.
Second, some patients find it difficult to coordinate the maneuver, in which
case there is no implication for a difficult intubation.
The upper lip bite test was proposed as a
modification of the TMJ displacement test. The upper lip bite test is performed
by asking the patient to move the mandibular incisors as high on the upper lip
as possible. The maneuver is similar to biting the lip. Contact of the teeth
above or on the vermilion border is thought to predict adequate laryngo-scopic
views. Inability to contact the vermilion border is thought to predict poor
laryngoscopic views. Both the TMJ translation test and the upper lip bite test
assess TMJ glide, which is an important consideration during laryngoscopy.
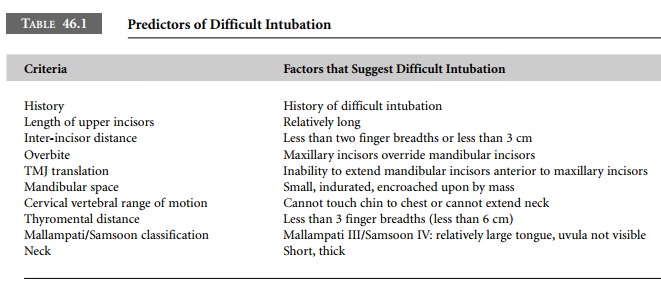
Table 46.1 summarizes a quick, easy, bedside scheme for predicting difficult
intubation.
Related Topics