Chapter: Clinical Cases in Anesthesia : Spine Surgery
Describe the effects of anesthetics on somatosensory and motor evoked potentials
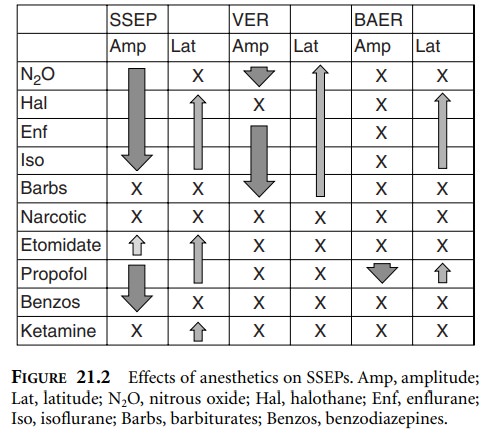
Describe
the effects of anesthetics on somatosensory and motor evoked potentials.
The EEG is sensitive to all anesthetics and
becomes markedly depressed at the upper end of the clinically relevant dosage
range, hence its use in monitoring depth of anesthesia. The anesthetic
technique that provides for hemodynamic stability and effective recording of
SSEPs and/or MEPs is obviously preferred. Inhalational agents
The inhalation response is generally dose-related; therefore a
low concentration with or without nitrous oxide and a continuous opioid
infusion is frequently utilized with success. Muscle relaxants do not interfere
with SSEP recording and may facilitate anesthetic management. If the potentials
remain difficult to obtain, changing to a total intravenous anesthesia (TIVA)
technique may be neces-sary. It is important to note that SSEPs are also
affected by ischemia, hypothermia, hypoxia, hypotension, and anemia.
While SSEPs are easily obtained using a low
concentra-tion of volatile agents and muscle relaxants, MEPs are more
challenging and often require the use of TIVA with minimal or no muscle relaxants. The inhalational
agents, including nitrous oxide, have been shown to depress MEPs in a variety
of circumstances. Intravenous anesthetic agents, such as propofol, midazolam,
droperidol, and sodium thiopental by infusion or bolus, may cause a significant
decrease in the amplitude or latency of MEPs. Ketamine and opioid analgesics,
such as fentanyl, produce less promi-nent changes. An opioid infusion with low
concentrations of propofol is a frequently successful technique for moni-toring
MEPs. Remifentanil is particularly useful because of its potency and
titratability. An intraoperative “wake-up test” may be requested if monitoring
is unavailable or inadequate.
Related Topics