Chapter: Essentials of Psychiatry: Time-limited Psychotherapy (Including Interpersonal Therapy)
Contraindication to Time-limited Psychotherapy
Contraindication
to Time-limited Psychotherapy
For all
psychoactive treatments it is important to consider instances in which a
specific therapy is not indicated
for a disorder or kind of patient. Unfortunately, thus far there are no
well-designed em-pirical studies of a psychotherapy’s potential “toxicities”,
although there is speculation about the kinds of individuals who would be
predicted to respond poorly to time-limited treatments
In the
brief psychodynamic psychotherapy literature, time-limited treatments are
generally not recommended for those individuals who might have difficulty in
quickly forming a thera-peutic alliance or might develop severe difficulties in
the face of termination (Marmor 1979). In practice, this usually translates
into a reluctance to treat borderline, suicidal, substance abusing, or
psychotic patients with brief psychotherapy (Davanloo, 1980; Mann, 1974;
Sifneos, 1979). Also excluded are “acting out”, cog-nitively impaired, very
dependent, or “unrestrainably” anxious patients (Koss and Shiang, 1994).
Although Sifneos (1979) and Mann (1974) consider severe psychopathology a contraindication to their brief psychodynamic psychotherapies, other time-limited treatments specifically tar-get serious mental disorders. IPT and CBT, for example, were developed for the treatment of major depression; these and other brief psychotherapies have been used to treat a spectrum of sig-nificant pathologies including bulimia (Fairburn, 1998), alcohol dependence (Miller et al., 1998), panic disorder (Barlow, 1997; Milrod et al., 2000), and post traumatic stress disorder (Foa et al., 1991)
Although
it is unlikely that a personality disorder will re-mit following a course of
brief psychotherapy, we also know that it is often difficult accurately to
diagnose personality disorders in the presence of an Axis I disorder
(Hirschfeld et al., 1983). Hence seeming Axis II pathology should rarely
be an exclusion in the presence of an appropriate Axis I target disorder.
Further-more, the structure and brevity of time-limited treatments may help the
therapist to manage or circumvent some of the treatment-interfering behaviors
characteristic of cluster B personality dis-orders. Thus, it may be reasonable
to treat patients with moderate character pathology for an Axis I disorder with
a TLP and then refer them for a different kind of psychotherapy once the acute
symptoms have remitted.
Empirical Data
Because
these treatments are relatively short, it is easier (though by no means easy)
to conduct psychotherapy outcome studies with TLPs than with longer-term
psychotherapies. The past decade has witnessed the publication of relatively
large numbers of TLP stud-ies. Because of these studies, we have more
confidence that TLPs work, at least for particular indications, than other
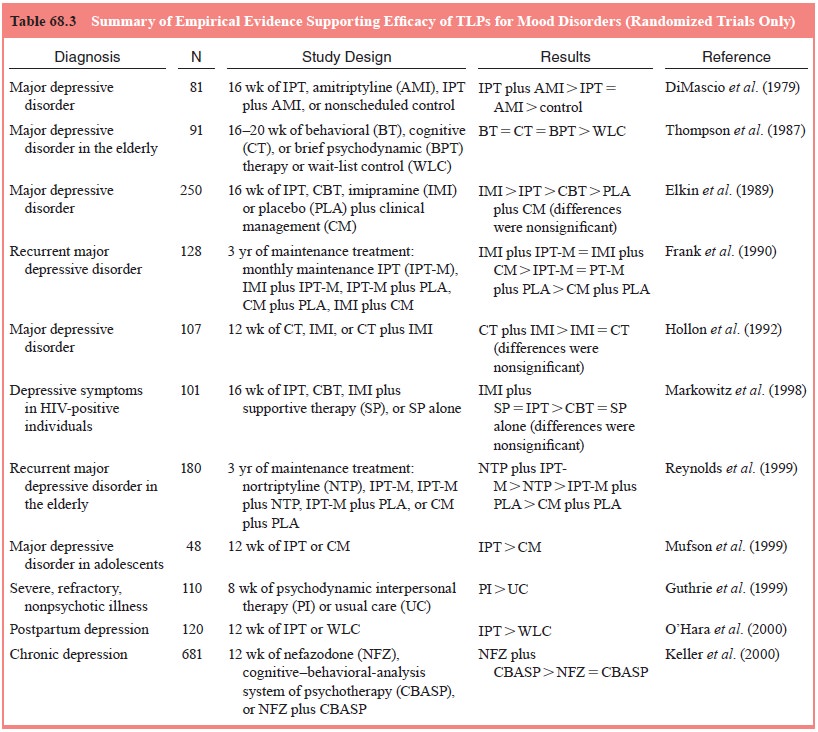
forms of psy-chotherapy. In Table 68.3, we summarize findings from empirical
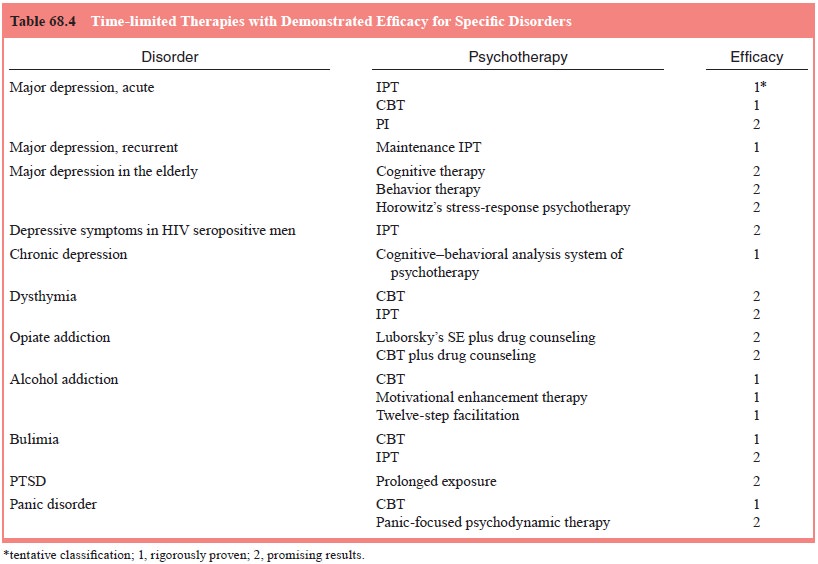
studies of TLPs as treatments for mood disorders. In Table 68.4 we summarize
population-specific indications for selected TLPs.
Related Topics