Chapter: Essentials of Psychiatry: Cognitive Psychology: Basic Theory and Clinical Implications
Cognitive Psychology: Anxiety Disorders
Anxiety Disorders
An individual in an anxious state gives heightened
attention to threat-related cues (MacLeod et
al., 1986; Matthews and MacLeod, 1985; Brosschot et al., 1999; Bradley et al.,
2000; Fox et al., 2001; Lundh and
Oest, 2001; Bradley et al., 1999;
Mogg et al., 2000), as such cues are
usually particularly salient to the feelings
of anxiety; this selectivity process may in turn filter out and discard
information not congruent with the anxious mood state. Such a mood-congruent
attentional bias helps orient the individual to the source of danger, which may
in turn help en-sure that the individual formulates an appropriate response to
the threatening situation. To the extent that there is a reasonable goodness of
fit between the level of anxious arousal and the level of genuine threat posed
to the individual by the environment, the mood-congruence attentional bias
serves an adaptive func-tion. When the level of anxiety is consistently
incommensurate with the environmental context, however, a state of pathological
anxiety ensues.
Barlow’s (1988) anxious apprehension model suggests that pathological anxiety, such as that observed in GAD, may arise from a chronic misapprehension or overestimation of the level of threat posed by a wide array of situations, many of them benign. It is further proposed that, once the anxious arousal of a patient with GAD is triggered by the misappre-hension of threat, there is a narrowing of external attention to the perceived danger, concurrent with a ruminative internal self-focus on negative expectancies regarding the situation’s outcome. Two deleterious consequences of such an attentional bias predictably ensue: 1) the patient disregards or discounts information that could serve to correct the original misappre-hension of threat and 2) the patient’s attentional resources are so thoroughly consumed by the focus on negative expectancies that few resources are available for constructive problem solv-ing and adaptive responding.
A somewhat related cognitive model of pathological
anxi-ety has been proposed by Beck and Emery (1985) in the schema theory of
anxiety. Central to this theory is the mechanism of cognitive appraisal, with
anxiety as the feeling state resulting from the appraisal of threatening
stimuli. The appraisal pro-cess, in turn, is believed to be influenced by
cognitive structures known as schemata, which consist of stored information
ab-stracted from previous experience (Dombeck and Ingram, 1993; Dibartolo et al., 1997). Schema-guided appraisal
is held to take place automatically.
Schema theory views pathological anxiety as the
result of faulty schemata that lead to habitual, and largely automatic,
overappraisal of danger; pathological appraisal often takes place automatically
without benefit of the scrutiny that accompanies attentional focus.
Accordingly, Beck’s therapeutic approach to ameliorating pathological anxiety
involves helping the patient allocate more attentional resources to the
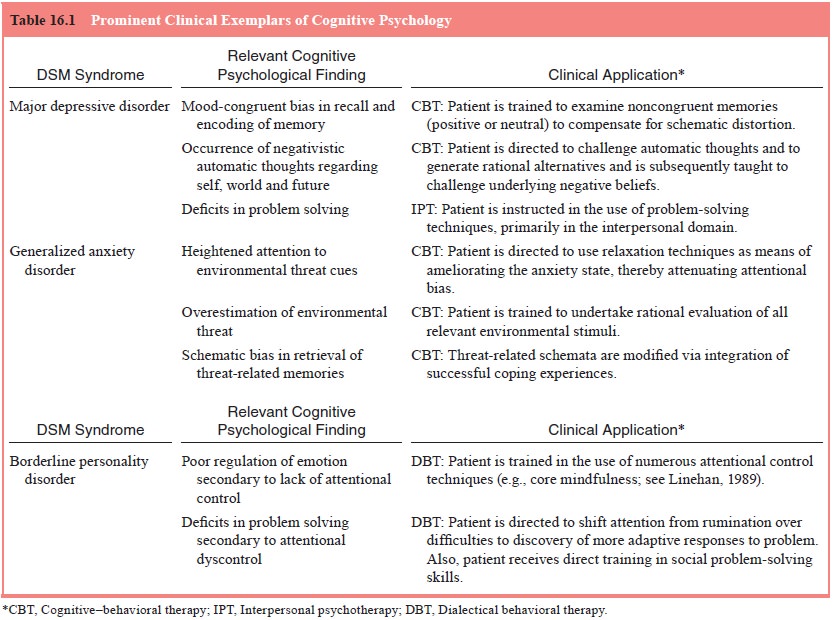
appraisal process, as a corrective to faulty schematic processing. Applications
from cognitive psychology to the treatment of anxiety disorders are presented
in Table 16.1
Related Topics