Chapter: Obstetrics and Gynecology: Hypertension in Pregnancy
Classification of Hypertension in Pregnancy
Hypertensive disorders occur in
approximately 12% H
to 22% of pregnancies and cause substantial peri-natal
morbidity and mortality for both mother and fetus. Hypertensive disease is
directly responsible for ap-proximately 20% of maternal
deaths in the United States. The exact cause of hypertension in pregnancy
remains unknown.
CLASSIFICATION
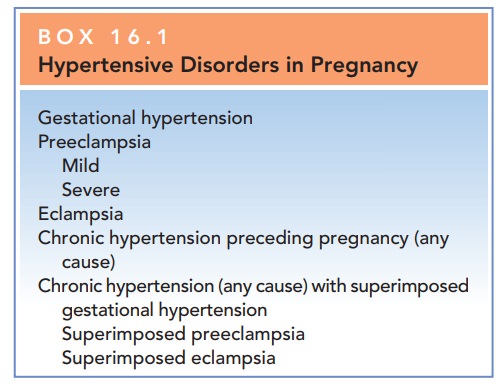
Various classifications of
hypertensive disorders in preg-nancy have been proposed. Box 16.1 presents a
commonly used classification. Because hypertensive disorders in preg-nancy
represent a spectrum of disease, classification systems should be used as a
guide only
Chronic Hypertension
Chronic hypertension is defined as hypertension
present beforethe 20th week of pregnancy or hypertension present before
preg-nancy. The categories of hypertension in pregnancy andthe
blood pressure (BP) criteria used to define each are as follows:
·
Mild hypertension: Systolic
pressure of >=140–180
mm Hg or diastolic pressure of >=90–100 mm
Hg or both
·
Severe hypertension: Systolic
pressure of >=180 mm Hg
or diastolic pressure of >=100 mm Hg
A major risk with chronic
hypertension is the development of preeclampsia or eclampsia later in the
pregnancy, which is relatively common and difficult to diagnose. The acute
onset of proteinuria and worsening hypertension in women with chronic
hypertension is suggestive of superimposed preeclampsia.
Preeclampsia
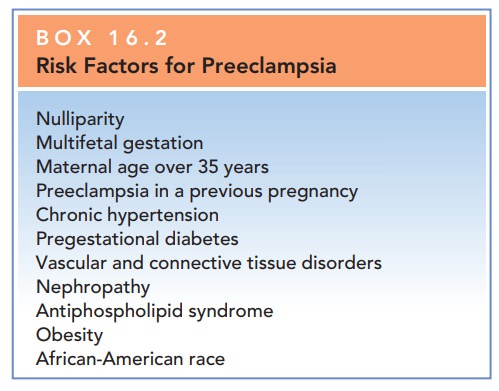
Preeclampsia is the development of
hypertension with protein-uria and edema after 20 weeks of gestation. This
condition canoccur earlier in the presence of gestational trophoblastic
disease. Risk factors for preeclampsia are in Box 16.2. The criteria for
diagnosis of preeclampsia are:
· Blood
pressure of >=140 mm Hg
systolic or >=90 mm Hg
diastolic that occurs after 20 weeks of gestation in a woman with previously
normal blood pressure
· Proteinuria,
defined as urinary excretion of 0.3 g protein or higher in a 24-hour urine
specimen
Severe
preeclampsia is characterized by one or more ofthe following:
·
Blood pressure >=160 mm Hg systolic or >=110 mm Hg diastolic on two
occasions at least 6 hours apart while the patient is on bed res
·
Marked proteinuria (generally >=5 g per 24-hour urine collection,
or 3+ or more
on two dipstick of random urine samples collected at least 4 hours apart)
·
Oliguria <500 mL in 24 hours
·
Cerebral or visual disturbances
such as headache and scotomata (“spots” before the eyes)
·
Pulmonary edema or cyanosis
·
Epigastric or
right-upper-quadrant pain (probably caused by subcapsular hepatic hemorrhage or
stretching of Glisson capsule)
·
Evidence of hepatic dysfunction
·
Thrombocytopenia
·
Intrauterine fetal growth
restriction (IUGR)
These changes illustrate the
multisystem involvement asso-ciated with preeclampsia. Severe preeclampsia is
an indica-tion for delivery, regardless of gestational age or maturity.
Eclampsia
Eclampsia is the additional presence of convulsions (grand mal seizures) in a woman with preeclampsia that is not explained by a neurologic disorder. Eclampsia occurs in 0.5% to 4%of patients with preeclampsia.
Most
cases of eclampsia occur within 24 hours of delivery, but approximately 3% of
cases are diagnosed between 2 and 10 days postpartum.
HELLP Syndrome
HELLP syndrome is the presence of hemolysis, elevated liverenzymes,
and low platelet count.
HELLP
syndrome, like severe preeclampsia, is an indication for delivery to avoid
jeopardizing the health of the woman.
This syndrome is now appreciated
as a distinct clinical en-tity, occurring in 4% to 12% of patients with severe
pre-eclampsia or eclampsia. Criteria for diagnosis are:
· Microangiopathic
hemolysis
· Thrombocytopenia
· Hepatocellular
dysfunction
Related Topics