Chapter: Essentials of Psychiatry: Childhood Disorders: Learning and Motor Skills Disorders
Childhood Disorders: Communication Disorders
Childhood Disorders: Communication Disorders
Definitions
Psychiatric practice depends upon communication and
language. Language and or learning disorders have been linked in the past, but
in DSM-IV-TR (American Psychiatric Association, 2000) they are regarded as
separate although often associated condi-tions. This section covers: Expressive
Language Disorder, Mixed Receptive-Expressive Language Disorders, Phonological
Disor-der, Stuttering and Communication Disorder NOS. These disor-ders share
many common features, as noted in Table 26.1. They are defined by criteria in
DSM-IV-TR. In all cases a test score or assessment measure alone does not
define these conditions. An individual must also experience social, academic or
occupational difficulties directly related to the condition.
DSM-IV-TR does not consider receptive language
disorders in isolation. Receptive language disorders in children seldom, if
ever, can occur without concurrent (and perhaps resultant) prob-lems with
expression. This is in direct contrast with such entities as Wernicke’s aphasia
in adults, which affect reception alone.

Outside of DSM-IV-TR, the term “phonologic
disorder” may refer to a condition characterized by difficulty in generat-ing
sound combinations, as for example in the case of laryngeal dysfunction.
Epidemiology
Prevalence
Prevalences varying from 1 to 13% have been
reported for lan-guage disorders, and numbers as high as 32% for speech
disorders (Baker, 1990). In development of the DSM-IV-TR, researchers found
that
·
Acquired language disorders appear less common than
the developmental types.
·
3–7% of all children were suspected of having a
developmen-tal Expressive Language Disorder.
·
Mixed Expressive – Receptive Language Disorder
appears in up to 3% of school-age children.
·
Phonological Disorder occurs in approximately 2% of
six and seven-year olds, falling to 0.5% by age 17.
·
Stuttering occurs in approximately 1% of children
10 and younger, declining to 0.8% in later adolescence.
·
All of these conditions have a male to female
predominance; that of stuttering is as high as 3 : 1.
Comorbidity
General
Cantwell and Baker (1991) demonstrated that
approximately half of the children with a speech or language disorder have some
other definable Axis I clinical disorder. Similarly, among children with a
psychiatric diagnosis first made, there is a remarkably increased likelihood of
speech and language disorders, which often go un-detected. Beitchman (1985)
found more than four times the preva-lence of psychiatric illness in
kindergartners with communication disorders compared with nondisordered
children. Cantwell and Baker also found that psychiatric illness in their
population was associated with greater severity of communication problems.
Conversely, the presence of communication disorders
may be associated with increased severity of some psychiatric conditions, most
notably the Disruptive Behavior Disorders. Physicians must recognize that these
disorders do not occur in an isolated context
Expressive Language Disorder and Mixed Receptive-expressive Language Disorder
Phonological Disorder and Learning Disorders are
common among children with this disorder. Other neurodevelopmental conditions
are also seen, such as motor delays, coordination disorders and enuresis,
although the rate of association is un-certain. These disorders and the
stresses they create frequently lead to Adjustment Disorders and social
withdrawal. Cantwell and Baker (1991) found that the most common psychiatric
disor-der among children with communication disorders overall was Attention Deficit
Hyperactivity Disorder (ADHD), representing 19% of their sample of 600 children
referred for a communi-cation evaluation. Some authors have speculated that
ADHD may be concordant with an entity known as Central Auditory Processing
Disorder (CAPD), which refers to deficits in the pro-cessing of audible
signals, and which can be subsumed under the DSM-IV language disorders. A total
concordance is unlikely, but Riccio et al.
(1994) suggest that 50% of children with CAPD also have ADHD.
Phonologic Disorder
Children with this problem may have clear causal
factors, such as anatomic, neurological, or cognitive disorders, al-though most
do not. They do have a higher prevalence of language disorders, with all their
associated problems, than do normal controls. They appear more likely to have
ADHD, though probably not as commonly as do children with lan-guage disorders.
Children with Phonological Disorders, es-pecially when associated with
stuttering or hyperactivity, are prone to social discrimination and isolation,
with subsequent consequences.
Stuttering
Other communication disorders are more frequently
reported in those with stuttering than in normal controls. Stuttering is
frequently accompanied by many linguistic mechanisms and social maneuvers to
avoid its manifestation, and is often exac-erbated by anxiety or stress.
Persons with stuttering face social discrimination. They have been mocked in
drama and cinema (including cartoons) for centuries, and all too often are
regarded as intellectually impaired.
Etiology and Pathophysiology
Genetic Influences
No clear mechanisms of genetic transmission have
been elu-cidated, but a number of instances of family aggregation have been
reported. At least one of these (Gopnik and Crago, 1991) suggested the presence
of a single dominant autosomal gene. Tomblin (1989) reported increased
concordance of language disorders among siblings. An increasing number of
family studies now suggest that these disorders are familial, includ-ing the
Twins Early Development Study (TEDS) in the United Kingdom (Plomin and Dale,
2000). These reports cannot ab-solutely prove any genetic hypothesis but are
provocative and suggest a polygenetic basis.
A genetic basis for stuttering has been proposed
for many years. The Yale Family Study of Stuttering suggested that 15% of first
degree relatives of probands are affected at some time in their lives (Kidd,
1983).
Pathophysiologic influences
Neurophysiological Factors
Communication disorders arise from at least three
interrelated sets of factors: neurophysiologic (including structural),
cogni-tive-perceptual and environmental. However, the great majority of
children with communication disorders exhibit no specific CNS damage, and thus
minimal or subclinical damage has been postulated. The relative frequency of
“soft” neurologic signs and lateral dominance problems in this population
provokes this speculation. However, no clear neurophysiologic mechanisms or
pathology can be correlated with these disorders. Some interest-ing findings
are emerging, including suggested anatomical dif-ferences in the left cerebral
cortex in stuttering, prenatal alcohol exposure and the physical sequelae of
abuse and neglect.
Cognitive and Perceptual Factors
Perceptual hypotheses relate communication
disorders to various deficits in the reception, acquisition, processing,
storage, or recall of different elements of communication. Table 26.2 notes
various perceptual deficits that have been implicated, including auditory
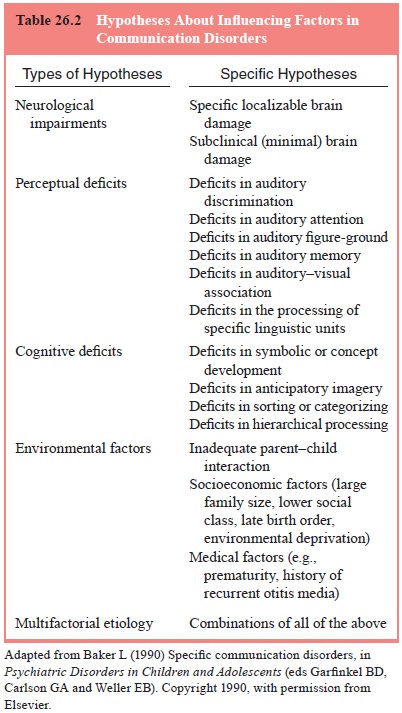
discrimination, attention, memory and visual
association. More purely cognitive hypotheses have also been proposed,
involving deficits in symbolization, categorizing, hierarchical processing and
related areas. Some authors (Friel-Patti, 1992; Helmuth, 2001) propose that
there are certain language-specific cognitive deficits. The special
phenomenology of stuttering suggests the possibility of dyssynchrony between
phonation and articulation, as reported by Perkins (2001).
Environmental Factors
This category refers both to the psychosocial
environment of the child and to general medical factors such as perinatal
complica-tions or recurrent otitis media.
The relationship of socioeconomic status to the
occurrence of communication disorders is uncertain. Variables such as class,
family size, income and birth order all clearly affect the amount of verbal
interaction children receive and have been implicated. The association between
the exacerbation of stuttering and stress is well known, although work in this
area has frequently con-founded predisposing, triggering and maintaining
factors.
Review of these influences reveals a considerable
amount of overlap, and clinical observation seldom if ever suggests a uni-tary
causality of Communication Disorders in real patients.
Related Topics