Chapter: Modern Pharmacology with Clinical Applications: Androgens, Antiandrogens, and Anabolic Steroids
Androgens: Clinical Uses
CLINICAL USES
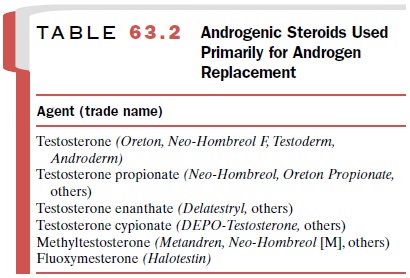
The primary therapeutic use
of androgens is as replace-ment therapy in testicular deficiency (Table 63.2),
a condition in which induction and maintenance of male secondary sex
characteristics are desired. Although replacement therapy is the primary use of
androgen ad-ministration, these hormones also are used and abused for their
protein anabolic effects.
Hypogonadism
Testicular failure may occur
before puberty and present as delayed puberty and the eunuchoid phenotype, or
af-ter puberty, with the development of infertility, impo-tence, or decreased
libido in otherwise fully virilized males. The source of hypogonadism can be
testicular, as occurs in primary
hypogonadism, or it may result from abnormalities of the
hypothalamic–pituitary axis, as in secondary
hypogonadism.
Prepuberal Hypogonadism
Prepuberal hypogonadism is often unsuspected until a delay in male sexual development is noticed at the time of puberty.
The eunuchoid
phenotype is caused by absent or deficient androgenic induction of the
undif-ferentiated embryonic bipotential tissue into fully de-veloped male sex
accessory organs. Causes of this con-dition include deficient testicular
steroidogenesis (both congenital and acquired), target organ androgen
insen-sitivity syndromes (receptor defects, 5 -reductase defi-ciency),
deficient pituitary LH and FSH secretion, or deficient hypothalamic GnRH
production. Androgen replacement therapy is effective only when the end or-gans
are sensitive to androgens, so certain forms of pseudohermaphroditism are
unresponsive to androgen replacement.
The compounds most effective in bringing about masculinization are
the long-acting enanthate, cypionate, or propionate esters of testosterone;
these preparations require intramuscular injection. Recently effective
cuta-neous forms of androgens have become available and may be equally
effective. Owing to inconsistent drug ab-sorption, oral androgen preparations
do not result in full sexual development in prepuberal hypogonado-tropic males.
Postpuberal Hypogonadism
Postpuberal hypogonadism is
also classified as either primary hypogonadism or secondary hypogonadism.
Primary hypogonadism occurs after puberty as the re-sult of surgical castration
or testicular destruction (e.g., through orchitis, radiation) and is associated
with ele-vated levels of LH and FSH. Secondary hypogonadism is usually
associated with hypopituitarism from destruc-tion or infiltration of the hypothalamus
or pituitary by infarction, tumoral replacement, or surgical removal.
Thus, these individuals have
inappropriately low LH and FSH levels that do not respond to GnRH stimula-tion.
Androgen replacement in these individuals usually restores secondary male
sexual characteristics, such as libido and potency.
Aging and Impotence
Aging in men is associated
with decreased testicular function that results in reduced testicular
steroidogene-sis, decreased free plasma testosterone levels, decreased 17-ketosteroid
excretion, and increased gonadotropin levels. Decreased testicular function has
been impli-cated as a cause of reduced libido, muscle mass, muscle strength,
and bone density in elderly men. However, these observations are so variable
that a causal rela-tionship between lowered androgen levels has not been firmly
established. Androgen replacement in
elderly men has not been demonstrated
to be beneficial unless there is true androgen deficiency. In addition, it
is wise to avoid the indiscriminate use
of androgens in this age group because of the high incidence of prostate
neoplasms (benign and malignant). Androgen administration in re-placement doses
has proved to be moderately success-ful in increasing libido and sexual
performance in men who have true testicular failure.
Anemia
Androgens stimulate
erythrocytosis and are effective in the treatment of certain anemias that are
secondary to endocrine hypofunction or myeloid hypoplasia. In high dosages,
these compounds in the past were used in the treatment of several forms of
anemia. However recom-binant erythropoietin has replaced the androgens as a
more effective treatment of most forms of anemia.
Therapeutic Use of Androgens in Women
Because of the antagonistic
action of androgens in many estrogen-sensitive tissues, it would seem logical
that androgens might be effective therapeutic agents in clinical situations of
estrogen excess or in the presence of estrogen-dependent neoplasms. However,
the viriliz-ing side effects of these
compounds have limited their clinical use. Selective protein anabolic forms
of andro-gens have been used in certain clinical situations.
Endometriosis
Endometriosis is abnormal growth of endometrial tissue in the peritoneal cavity. Women with this disorder have dysmenorrhea,
dyspareunia, chronic pelvic pain, and in-fertility. Danazol (Danocrine) is a 2,3-isoxazol deriva-tive
of 17 -ethynyl testosterone (ethisterone) that has weak virilizing and protein
anabolic properties. It is ef-fective in endometriosis through its negative
feedback inhibition of LH and FSH release, which in turn results in decreased
ovarian steroidogenesis and regression of endometriomas. Because of the
virilizing side effects of danazol, causing acne and hirsutism, its use in
en-dometriosis has been largely supplanted by the use of GnRH analogues.
Danazol is also approved for use in fi-brocystic breast disease and hereditary
angioneurotic edema.
Female Hypogonadism
Female hypogonadism,
especially prepuberal, may be an indication for androgen therapy. Androgens are
nec-essary for normal pubic hair induction and long bone growth in both sexes.
In prepuberal females with hy-popituitarism in whom all other hormonal
deficiencies (estrogen, progesterone, thyroid, adrenal, and growth hormone)
have been corrected, normal sexual develop-ment and long bone growth are not
complete without androgen hormone replacement. Estrogen administra-tion during
adolescence is necessary for the develop-ment of the breast, the gynecoid
pelvis, and other fe-male characteristics. However, maximal long bone growth
and development of axillary and pubic hair will not occur without small amounts
of androgen replace-ment. The use of methyltestosterone
(Android) and di-ethylstilbestrol in combination has been demonstrated to be very effective in inducing
complete secondary sex-ual development in these females. Finally, low doses of
androgens have been used to facilitate impaired libido in postmenopausal women
when combined with estro-gen replacement therapy.
Use of Androgens as Protein Anabolic Agents
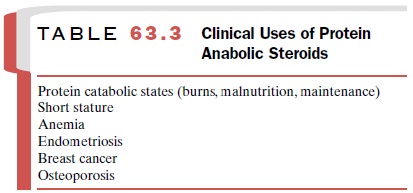
Anabolic activities of testosterone, such as increases in amino acid incorporation into protein and in RNA polymerase activity, have been demonstrated in skeletal muscle. Apart from the direct anabolic effects in specific tissue, androgens antagonize the protein catabolic ac-tion of glucocorticoids. The androgen compounds with the greatest ratio of protein anabolic effects to virilizing effects are the 19-nortestosterone derivatives. Compounds that are used clinically (Table 63.3) include nandrolone phenpropionate (Durabolin), nandrolone decanoate (Deca-Durabolin), methandrostenolone (Dianabol), oxymetholone (Anadrol, Adroyd), stanozolol (Winstrol), and oxandrolone (Anavar).
The protein anabolic
compounds are most com-monly used to stimulate appetite and muscle mass in
persons with advanced malignancy or other conditions characterized by advanced
malnutrition. These com-pounds are also often abused by athletes who are trying
to build muscle mass. Athletes often take multiple com-pounds at the same time
(stacking) or sequentially to try to maximize their anabolic effects. This type
of use is not based on scientific data but rather on hyperbole of-ten spread by
individuals with no medical or scientific background. Athletes who use these
compounds in this way are unaware of the potential adverse effects or do not
care.
Related Topics