Chapter: Pathology: Endocrine Pathology
Adrenal Gland - Pathology
ADRENAL GLAND
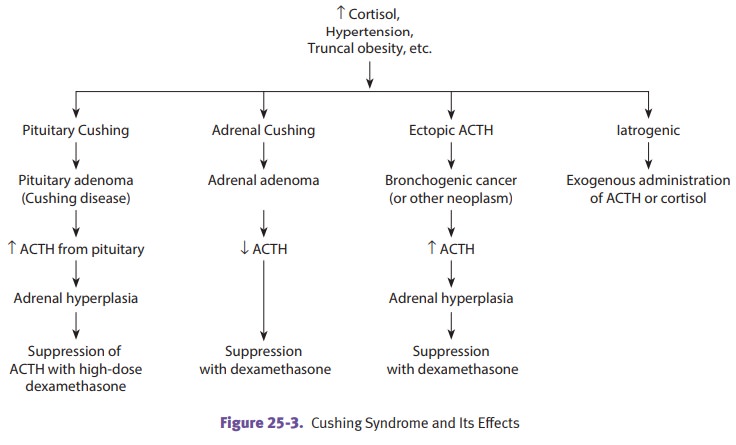
Cushing syndrome is characterized by increased
levels of glucocorticoids. It is inves-tigated with lab and imaging studies.
The most com-mon cause is exogenous glucocorticoid administration.
Endogenous causes include:
•
Cushing disease (hypersecretion of ACTH, usually due to a pituitary
micro-adenoma)
•
Secretion of ACTH from nonpituitary tumors (e.g., small cell lung
cancer)
•
ACTH-independent Cushing syndrome due to adrenal neoplasia
Clinical manifestations
include hypertension, weight gain (truncal obesity, “buf-falo hump” and moon
facies), cutaneous striae, hirsutism and mental disturbances.
Hyperaldosteronism may cause hypertension and
hypokalemia.
•
Primary (decreased plasma renin)
°°
Adrenocortical neoplasm: adenoma (Conn syndrome)
■■ Circumscribed yellow nodule
with vacuolated cells
■■ Carcinoma: poorly demarcated
lesion with cystic change and pleomorphic cells
°°
Bilateral nodular hyperplasia of the adrenal
•
Secondary (increased plasma renin)
(e.g., renal artery stenosis)
Adrenogenital syndromes are adrenal disorders
characterized by excess production of androgens and virilization. They are caused
either by adrenocortical adenoma/ carcinoma, which produces androgens, or by
congenital adrenal hyperplasia, a cluster of autosomal recessive enzyme defects
(most common is 21-hydroxylase deficiency).
Waterhouse-Friderichsen syndrome (acute adrenal insufficiency)
is a potentially fatal, bilateral hemorrhagic
infarction of the adrenal glands associated with sepsis, often due to a N. meningitidis infection in children.
It is clinically characterized by disseminated intravascular coagulation (DIC),
acute respiratory distress syndrome, hypotension and shock, and acute adrenal
insufficiency. Treatment is antibiotics and steroid replacement.
Addison’s disease (chronic adrenocortical
insufficiency) is caused by destruction of the adrenal cortex,
leading to a deficiency of glucocorticoids, mineralocorticoids, and androgens.
The most common cause is autoimmune adrenalitis, though adrenal involvement by
TB or metastatic cancer are other possible causes. Patients present with
gradual onset of weakness, skin hyperpigmentation, hypotension, hypoglyce-mia,
poor response to stress, and loss of libido. Treatment is steroid replacement.
Secondary adrenocortical insufficiency may be caused by disorders of the hypo-thalamus
or pituitary (cancer or infection, for example). Since ACTH levels are low,
hyperpigmentation does not occur.
Pheochromocytoma (“dark/dusky-colored tumor”) is an uncommon benign tumor of the adrenal
medulla, which produces catecholamines (norepinephrine and epineph-rine). It
can present with sustained or episodic hypertension and associated severe
headache, tachycardia, palpitations, diaphoresis, and anxiety. Note the rule of
10s:
•
10% occur in children
•
10% are bilateral
•
10% are malignant
•
10% are familial (MEN 2A and 2B)
•
10% occur outside the adrenal gland
Urinary vanillylmandelic acid
(VMA) and catecholamines are elevated. Microscopi-cally, the tumor shows nests
of cells (Zellballen) with abundant cytoplasm. Treat-ment is control of the
patient’s BP and surgical removal of the tumor.
Related Topics