Chapter: Medical Physiology: Heart Valves and Heart Sounds; Dynamics of Valvular and Congenital Heart Defects
Valvular Lesions - Heart Sounds
Valvular Lesions
Rheumatic Valvular Lesions
By far the greatest number of valvular lesions results from rheumatic fever. Rheumatic fever is an autoim-mune disease in which the heart valves are likely to be damaged or destroyed. It is usually initiated by strep-tococcal toxin in the following manner.
The sequence of events almost always begins with a preliminary streptococcal infection caused specifically by group A hemolytic streptococci. These bacteria ini-tially cause a sore throat, scarlet fever, or middle ear infection. But the streptococci also release several dif- ferent proteins against which the person’s reticuloen-dothelial system produces antibodies. The antibodies react not only with the streptococcal protein but also with other protein tissues of the body, often causing severe immunologic damage. These reactions continue to take place as long as the antibodies persist in the blood—1 year or more.
Rheumatic fever causes damage especially in certain susceptible areas, such as the heart valves. The degree of heart valve damage is directly correlated with the concentration and persistence of the anti-bodies.
In rheumatic fever, large hemorrhagic, fibrinous, bulbous lesions grow along the inflamed edges of the heart valves. Because the mitral valve receives more trauma during valvular action than any of the other valves, it is the one most often seriously damaged, and the aortic valve is second most fre-quently damaged. The right heart valves, the tricuspid and pulmonary valves, are usually affected much less severely, probably because the low-pressure stresses that act on these valves are slight compared with the high-pressure stresses that act on the left heart valves.
Scarring of the Valves. The lesions of acute rheumaticfever frequently occur on adjacent valve leaflets simul-taneously, so that the edges of the leaflets become stuck together. Then, weeks, months, or years later, the lesions become scar tissue, permanently fusing por-tions of adjacent valve leaflets. Also, the free edges of the leaflets, which are normally filmy and free-flapping, often become solid, scarred masses.
A valve in which the leaflets adhere to one another so extensively that blood cannot flow through it nor-mally is said to be stenosed. Conversely, when the valve edges are so destroyed by scar tissue that they cannot close as the ventricles contract, regurgitation (back-flow) of blood occurs when the valve should be closed. Stenosis usually does not occur without the coexis-tence of at least some degree of regurgitation, and vice versa.
Other Causes of Valvular Lesions. Stenosis or lack of oneor more leaflets of a valve also occurs occasionally as a congenital defect. Complete lack of leaflets is rare; congenital stenosis is more common.
Heart Murmurs Caused by Valvular Lesions
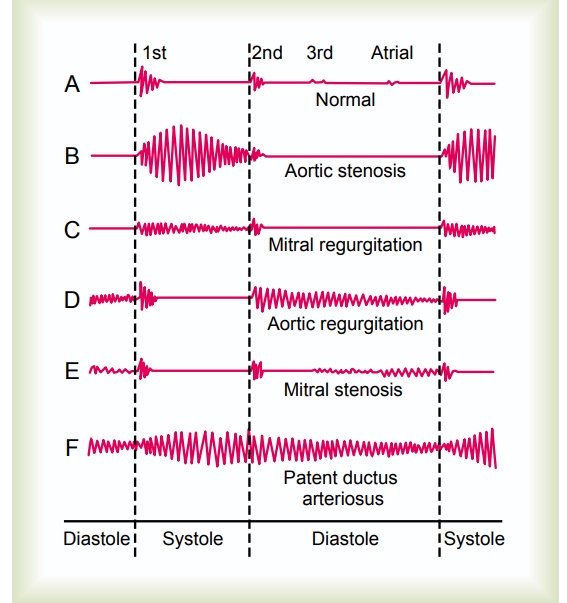
As shown by the phonocardiograms in Figure 23–3, many abnormal heart sounds, known as “heart murmurs,” occur when there are abnormalities of the valves, as follows.
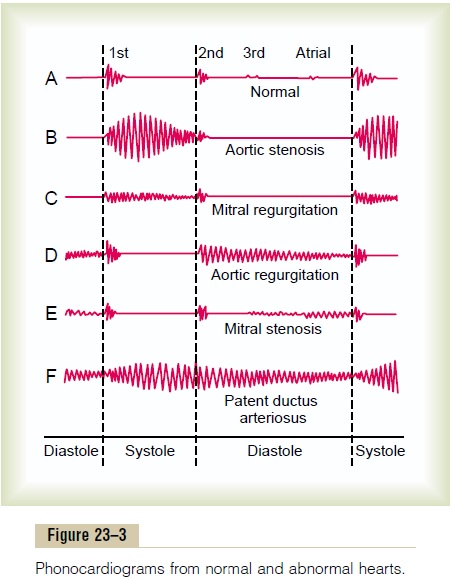
Systolic Murmur of Aortic Stenosis. In aortic stenosis,blood is ejected from the left ventricle through only a small fibrous opening of the aortic valve. Because of the resistance to ejection, sometimes the blood pres-sure in the left ventricle rises as high as 300 mm Hg, while the pressure in the aorta is still normal. Thus, a nozzle effect is created during systole, with blood jetting at tremendous velocity through the small opening of the valve. This causes severe turbulence of the blood in the root of the aorta. The turbulent blood impinging against the aortic walls causes intense vibra-tion, and a loud murmur (see recording B, Figure 23–3) occurs during systole and is transmitted throughout the superior thoracic aorta and even into the large arteries of the neck. This sound is harsh and in severe stenosis may be so loud that it can be heard several feet away from the patient. Also, the sound vibrations can often be felt with the hand on the upper chest and lower neck, a phenomenon known as a “thrill.”
Diastolic Murmur of Aortic Regurgitation. In aortic regurgi-tation, no abnormal sound is heard during systole, but during diastole, blood flows backward from the high-pressure aorta into the left ventricle, causing a “blowing” murmur of relatively high pitch with a swishing quality heard maximally over the left ventri-cle (see recording D, Figure 23–3). This murmur results from turbulence of blood jetting backward into the blood already in the low-pressure diastolic left ventricle.
Systolic Murmur of Mitral Regurgitation. In mitral regurgi-tation, blood flows backward through the mitral valve into the left atrium during systole. This also causes a high-frequency “blowing,” swishing sound (see record-ing C, Figure 23–3) similar to that of aortic regurgita-tion but occurring during systole rather than diastole. It is transmitted most strongly into the left atrium. However, the left atrium is so deep within the chest that it is difficult to hear this sound directly over the atrium. As a result, the sound of mitral regurgitation is transmitted to the chest wall mainly through the left ventricle to the apex of the heart.
Diastolic Murmur of Mitral Stenosis. In mitral stenosis,blood passes with difficulty through the stenosed mitral valve from the left atrium into the left ventri-cle, and because the pressure in the left atrium seldom rises above 30 mm Hg, a large pressure differential forcing blood from the left atrium into the left ventri-cle does not develop. Consequently, the abnormal sounds heard in mitral stenosis (see recording E, Figure 23–3) are usually weak and of very low frequency, so that most of the sound spectrum is below the low-frequency end of human hearing.
During the early part of diastole, a left ventricle with a stenotic mitral valve has so little blood in it and its walls are so flabby that blood does not reverberate back and forth between the walls of the ventricle. For this reason, even in severe mitral stenosis, no murmur may be heard during the first third of diastole. Then, after partial filling, the ventricle has stretched enough for blood to reverberate, and a low rumbling murmur begins.
Phonocardiograms of Valvular Murmurs. Phonocardio-grams B, C, D, and E of Figure 23–3 show, respectively, idealized records obtained from patients with aortic stenosis, mitral regurgitation, aortic regurgitation, and mitral stenosis. It is obvious from these phonocardio-grams that the aortic stenotic lesion causes the loudest murmur, and the mitral stenotic lesion causes the weakest. The phonocardiograms show how the inten-sity of the murmurs varies during different portions of systole and diastole, and the relative timing of each murmur is also evident. Note especially that the murmurs of aortic stenosis and mitral regurgitation occur only during systole, whereas the murmurs of aortic regurgitation and mitral stenosis occur only during diastole. If the reader does not understand this timing, extra review should be undertaken until it is understood.
Related Topics