Chapter: Basic & Clinical Pharmacology : Sulfonamides,Trimethoprim,& Quinolones
Trimethoprim & Trimethoprim-Sulfamethoxazole Mixtures - Antifolate Drugs
TRIMETHOPRIM & TRIMETHOPRIM-SULFAMETHOXAZOLE MIXTURES
Mechanism of Action
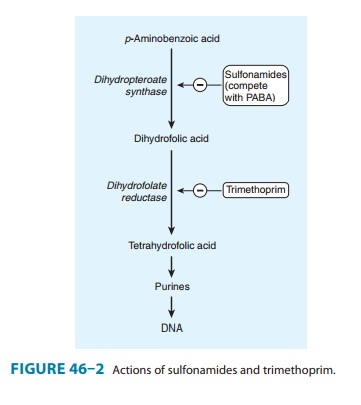
Trimethoprim, a trimethoxybenzylpyrimidine, selectively inhibits bacterial dihydrofolic acid reductase, which converts dihydrofolic acid to tetrahydrofolic acid, a step leading to the synthesis of purines and ultimately to DNA (Figure 46–2). Trimethoprim is about 50,000 times less efficient in inhibition of mammalian dihydrofolic acid reductase. Pyrimethamine, another benzylpy-rimidine, selectively inhibits dihydrofolic acid reductase of proto-zoa compared with that of mammalian cells. As noted above, trimethoprim or pyrimethamine in combination with a sulfon-amide blocks sequential steps in folate synthesis, resulting in marked enhancement (synergism) of the activity of both drugs. The combination often is bactericidal, compared with the bacte-riostatic activity of a sulfonamide alone.
Resistance
Resistance to trimethoprim can result from reduced cell permea-bility, overproduction of dihydrofolate reductase, or production of an altered reductase with reduced drug binding. Resistance can emerge by mutation, although more commonly it is due to plas-mid-encoded trimethoprim-resistant dihydrofolate reductases. These resistant enzymes may be coded within transposons on conjugative plasmids that exhibit a broad host range, accounting for rapid and widespread dissemination of trimethoprim resis-tance among numerous bacterial species
Pharmacokinetics
Trimethoprim is usually given orally, alone or in combination with sulfamethoxazole, which has a similar half-life. Trimethoprim-sulfamethoxazole can also be given intravenously. Trimethoprim is well absorbed from the gut and distributed widely in body fluids and tissues, including cerebrospinal fluid.
Because trimethoprim is more lipid-soluble than sulfamethox-azole, it has a larger volume of distribution than the latter drug. Therefore, when 1 part of trimethoprim is given with 5 parts of sulfamethoxazole (the ratio in the formulation), the peak plasma concentrations are in the ratio of 1:20, which is optimal for the combined effects of these drugs in vitro. About 30–50% of the sulfonamide and 50–60% of the trimethoprim (or their respec-tive metabolites) are excreted in the urine within 24 hours. The dose should be reduced by half for patients with creatinine clear-ances of 15–30 mL/min.Trimethoprim (a weak base) concentrates in prostatic fluid and in vaginal fluid, which are more acidic than plasma. Therefore, it has more antibacterial activity in prostatic and vaginal fluids than many other antimicrobial drugs.
Clinical Uses
A. Oral Trimethoprim
Trimethoprim can be given alone (100 mg twice daily) in acute urinary tract infections. Many community-acquired organisms are susceptible to the high concentrations that are found in the urine (200–600 mcg/mL).
B. Oral Trimethoprim-Sulfamethoxazole (TMP-SMZ)
A combination of trimethoprim-sulfamethoxazole is effective treatment for a wide variety of infections including P jirovecipneumonia, shigellosis, systemic salmonella infections, urinary tract infections, prostatitis, and some nontuberculous mycobacte-rial infections. It is active against most Staphylococcus aureus strains, both methicillin-susceptible and methicillin-resistant, and against respiratory tract pathogens such as pneumococcus, Haemophilus sp, Moraxella catarrhalis, and K pneumoniae (but not Mycoplasma pneumoniae). However, the increasing prevalence ofstrains of E coli(up to 30% or more) and pneumococci that are resistant to trimethoprim-sulfamethoxazole must be considered before using this combination for empiric therapy of upper uri-nary tract infections or pneumonia.One double-strength tablet (each tablet contains trimethoprim 160 mg plus sulfamethoxazole 800 mg) given every 12 hours is effective treatment for urinary tract infections and prostatitis. One half of the regular (single-strength) tablet given three times weekly for many months may serve as prophylaxis in recurrent urinary tract infections of some women. One double-strength tablet every 12 hours is effective treatment for infections caused by susceptible strains of shigella and salmonella. The dosage for children treated for shigellosis, urinary tract infection, or otitis media is 8 mg/kg trimethoprim and 40 mg/kg sulfamethoxazole every 12 hours.
Infections with P jiroveci and some other pathogens can be treated orally with high doses of the combination (dosed on the basis of the trimethoprim component at 15–20 mg/kg/d) or can be prevented in immunosuppressed patients by one double-strength tablet daily or three times weekly.
C. Intravenous Trimethoprim-Sulfamethoxazole
A solution of the mixture containing 80 mg trimethoprim plus 400 mg sulfamethoxazole per 5 mL diluted in 125 mL of 5% dextrose in water can be administered by intravenous infusion over 60–90 minutes. It is the agent of choice for moderately severe to severe pneumocystis pneumonia. It may be used for gram-negative bacterial sepsis, including that caused by some multidrug-resistant species such as enterobacter and serratia; shigellosis; typhoid fever; or urinary tract infection caused by a susceptible organism when the patient is unable to take the drug by mouth. The dosage is 10–20 mg/kg/d of the trimethoprim component.
D. Oral Pyrimethamine with Sulfonamide
Pyrimethamine and sulfadiazine have been used for treatment of leishmaniasis and toxoplasmosis. In falciparum malaria, the com-bination of pyrimethamine with sulfadoxine (Fansidar) has been used .
Adverse Effects
Trimethoprim produces the predictable adverse effects of an antifolate drug, especially megaloblastic anemia, leukopenia, and granulocy-topenia. The combination trimethoprim-sulfamethoxazole may cause all of the untoward reactions associated with sulfonamides. Nausea and vomiting, drug fever, vasculitis, renal damage, and cen-tral nervous system disturbances occasionally occur also. Patients with AIDS and pneumocystis pneumonia have a particularly high frequency of untoward reactions to trimethoprim-sulfamethoxazole, especially fever, rashes, leukopenia, diarrhea, elevations of hepatic aminotransferases, hyperkalemia, and hyponatremia.
Related Topics