Chapter: Essential Anesthesia From Science to Practice : Clinical management : The anesthesia machine
Systems with carbon dioxide absorption - The anesthesia machine
Systems with carbon dioxide
absorption
In
anesthesia, because of the cost (and ozone-depleting qualities) of volatile
anes-thetic agents, we prefer to conserve even more gas. Furthermore, the
patient does not consume all inhaled oxygen (at rest, a patient consumes only a
small por-tion of the inhaled oxygen, reducing the FiO2 of 0.21 to
an FeO2 of 0.17). Thus, we save a lot if we have to do nothing more
than replace the oxygen the patient consumes (for the average adult at rest –
about 250 to 300 mL/min). We need to remove the carbon dioxide, of which our
resting patient generates about as much (depending on his respiratory quotient)
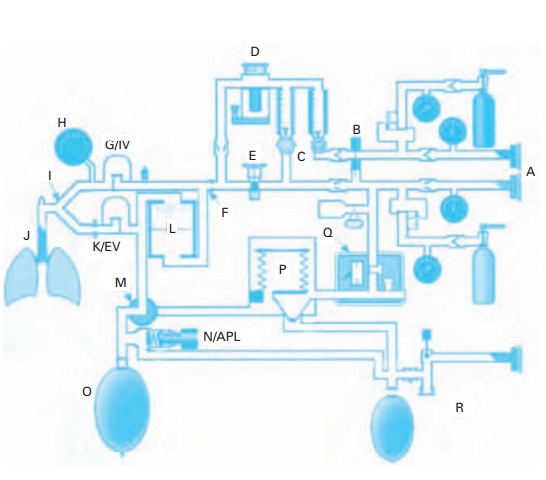
as he consumes oxygen. Figure 8.7shows the
arrangement. We simply formed a circle (conceptually, if not diagrammati-cally)
by connecting the expiratory and inspiratory limbs. The two valves in the
circle assure a one-way flow of gases in the circuit. We still have the APL
valve and the breathing bag, but we have incorporated a carbon dioxide
absorber. Now we can reduce the inflow of oxygen (and anesthetic gases) into
the circle quite drastically.
With
this circle system, we have the basic anesthesia machine. Now, all we need to
add are flow meters for other gases (nitrous oxide, air) and vaporizers that
let us introduce anesthetic vapor to the fresh gas flowing into the breathing
system. We also have the option of switching on a mechanical ventilator.
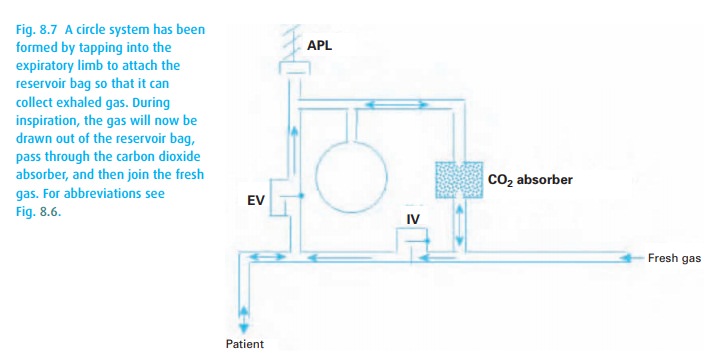
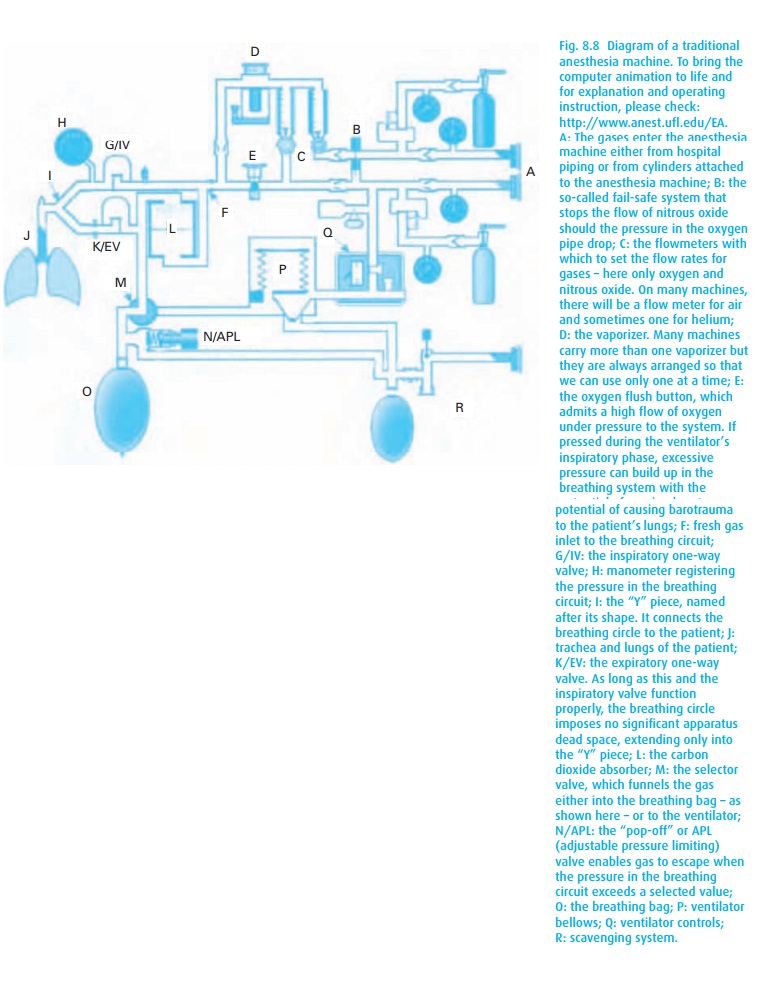
Using a handy diagram of a modern anesthesia machine (Fig. 8.8), we point out several features. The system receives compressed gases from the hospital’s gas supply; it has a back-up gas supply stored in cylinders; it reduces the high pres-sure in the cylinders to manageable levels in the machine; it has adjustable vapor-izers for halogenated anesthetics (isoflurane, desflurane and sevoflurane – but permits only one agent to be administered at a time); and it funnels the anesthetic-laden fresh gas into the breathing circuit that has a carbon dioxide absorber.
The system makes it possible for the patient to breathe spontaneously
into a breath-ing bag, which can be manually compressed if necessary, to
ventilate the patient’s lungs. While all systems have mechanical ventilators,
the design of these differs markedly among manufacturers of anesthesia
machines.
The
hospital system also provides suction that removes waste gases. Such
scav-enging keeps the air in the operating room virtually free of anesthetic
agents presumed to present a hazard to personnel, particularly pregnant women.
Modern
anesthesia machines have a bevy of safety features:
·
All gas hoses have connectors specific to the gas. This makes a
mix-up of gases unlikely. It does not guarantee that oxygen comes out of the
oxygen pipeline should the pipes have been switched during construction or
repairs, an occur-rence not all that rare.
·
One-way valves prevent gas from flowing from the cylinders into the
anesthe-sia machine as long as the system is connected to the pipeline. The
pipeline pressure exceeds the reduced cylinder pressure. This arrangement
prevents drainage of the cylinders while the machine is connected to wall
supply. This also means that one has to disconnect the machine from the wall
should it become necessary to use gas from the cylinders.
·
A safety valve closes the flow of nitrous oxide should the pressure
in the oxy-gen conduit drop below a critical level. This so-called fail-safe valve makes it impossible to
give nitrous oxide without pressure in the oxygen conduits.
·
A back-up to the fail-safe valve is the linkage between nitrous
oxide and oxygen, which prevents the delivery of less than 25% oxygen.
·
The gases in the breathing system are monitored and their
concentration dis-played.
The
machine depicted diagrammatically in Fig. 8.8can
be brought to life by sign-ing on to the Internet under
http://www.anest.ufl.edu/EA. There we can manip-ulate controls, operate the
ventilator, and watch the flow of color-coded gases. We can even cause the
system to have faults and observe the consequences. With the animated diagrams
comes a workbook that will not only explain features of the machine but also offer
self-tests.
Anesthesia
breathing circuits have come a long way since the open-drop ether days;
however, with increased sophistication also comes a need for heightened
awareness. These systems, if improperly used, e.g., inadequate fresh gas flow,
inappropriately tightened APL valve, faulty expiratory valve, incorrect setting
of the ventilator, undiscovered disconnection, can and do cause significant
injury. Because of these many potential dangers, we monitor gas flows,
pressures in the breathing circle, tidal and minute volumes, inspired oxygen,
and inhaled and exhaled carbon dioxide. Many of these variables come with
alarms that sound at adjustable thresholds.
Related Topics