Chapter: Pathology: Joint Pathology
Rheumatoid Arthritis
RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is
a systemic, chronic, inflammatory disease character-ized by progressive
arthritis, production of rheumatoid factor, and extra-articular manifestations.
It affects females 4x more than men, with highest incidence at ages 20–50. Some
cases have a genetic predisposition (HLA-DR4 and -DR1).
RA is thought to be caused by
an autoimmune reaction triggered by an infectious agent in a genetically
susceptible individual.
RA most commonly affects the
hand, wrist, knee, and ankle joints, and the involve-ment tends to be
symmetrical. There is often morning stiffness which improves with activity.
•
There is typically fusiform swelling, redness, and warmth of the
proximal interphalangeal (PIP) joint.
•
X-ray studies show juxta-articular osteoporosis and bone erosions;
joint effu-sion may also be present.
•
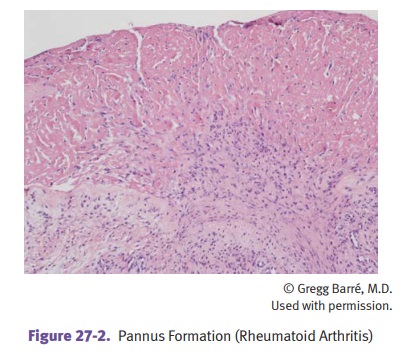
RA causes a diffuse proliferative synovitis, pannus formation
(proliferation of the synovium and granulation tissue over the articular
cartilage of the joint), fibrous and bony ankylosis (joint fusion), and joint
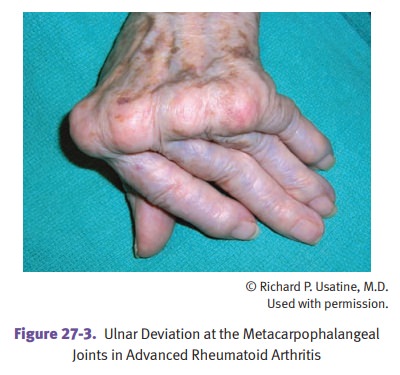
deformities. Joint deformities can include:
§ Radial deviation of the wrist
and ulnar deviation of the fingers
§ Swan neck deformity
(hyperextension of PIP joint and flexion of DIP joint
§ Boutonniere deformity
(flexion of PIP and extension of DIP joints)
•
Baker cysts (synovial cysts in the popliteal fossa) may be present.
Lab studies show elevated
sedimentation rate and hypergammaglobulinemia. Rheu-matoid factor (RF) is an
autoantibody (usually IgM) against the Fc fragment of IgG; it is present in 80%
of cases. RF may circulate and form immune complexes, and titer of RF
correlates with the severity of the arthritis and prognosis.
•
Extra-articular manifestations may be prominent. Systemic symptoms
include low-grade fever, malaise, fatigue, lymphadenopathy, and weakness.
Arteries may show acute necrotizing vasculitis due to circulating
antigen-antibody complexes.
•
Rheumatoid nodules, subcutaneous skin nodules, are present in 25%
of cases.
They are usually found on extensor surfaces of
the forearms and elbows, but can also be found in the heart valves, lung,
pleura, pericardium, and spleen. They are composed of central fibrinoid
necrosis surrounded by epithelioid macrophages, lymphocytes, and granulation
tissue.
•
Sjögren syndrome may be present in 15%. In Felty syndrome, RA
accompanies splenomegaly and neutropenia. In Caplan syndrome, RA is associated
with pneumoconiosis.
•
Secondary amyloidosis may also complicate RA.
Related Topics