Chapter: Essentials of Psychiatry: Relational Problems
Relational Problems
Relational Problems
Introduction
A
relational problem is a situation in which two or more emo-tionally attached
individuals (i.e., family members, romantic partners) engage in communication
or behavior patterns that are destructive or unsatisfying, or both, to one or
more of the indi-viduals. Relational problems deserve clinical attention
because, once initiated, they tend to be perpetuating and chronic, and are
frequently contemporaneous with or are followed by other seri-ous problems,
such as individual symptoms in the most vulnera-ble members of the family
(e.g., depression) or social unit dissolu-tion (e.g., divorce). They may be
diagnosed either in the presence or absence of individual disorders given in
the Diagnostic and Statistical Manual of Mental Disorders (DSM).
The
strength and direction of causality between the indi-vidual and the relational
problem are empirically undetermined. Few empirical investigations of the
relational problems that are “precursors” to individual pathology have been
conducted. Most of the existing research selects disturbed family units in
which one member has an existing disorder (e.g., schizophrenia, de-pression)
and examines the communication difficulties that ac-company the disorder. Thus,
cause-and-effect relations between individual disorders and relational
difficulties have not been ex-perimentally specified.
There is
also the issue of generalization: Do those who manifest relational problems
with a spouse or other family mem-ber manifest these same problems with others
and in other con-texts? Only a beginning literature exists on this issue.
However, preliminary data suggest that some individuals manifest severe
communication difficulties with their spouses or other family members but not
with persons outside the family.
Definition
Relational
problems are placed in the fourth edition of the DSM (DSM-IV-TR) section on
“other conditions that may be a focus of clinical attention”. Five specific
relational problems are described chiefly in terms of patterns of impaired
family interaction related to:
o
a mental or general medical condition
o
parent–child problem
o
partner
o
sibling
o
not otherwise specified (e.g. difficulties with
others outside of the family).
Constructs and Manifestations of Relational Problems
The
empirical data substantiate the existence of relational dif-ficulties that can
be reliably assessed and have clinical signifi-cance. The data are sparse in
reference to each DSM disorder and coexisting family relational difficulties,
with the exceptions of depression and schizophrenia.
In our
examination of the construct of relational problems, we emphasize those
constructs that have shown reliable assess-ment in research and that have been
found to 1) distinguish dis-tressed from nondistressed couples or families, or
2) to identify couples or families in which one or more members manifest
sig-nificant individual pathologic conditions.
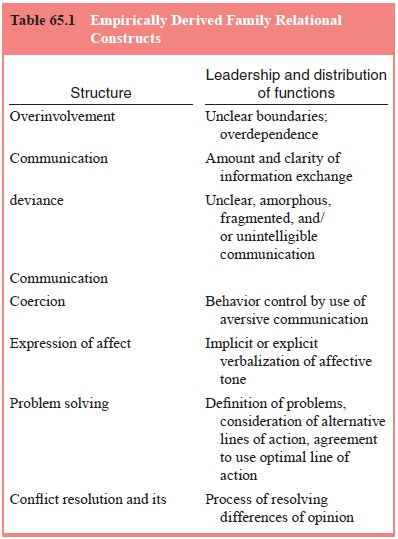
Four
major constructs (Table 65.1) have been investigated that describe nodal areas
of relational difficulty in the family and marital environment: structure, communication,
expression of affect and problem solving. Relational difficulties in other
environments (e.g., work) have not been described in the clinical literature.
It is
interesting to compare the constructs investigated in the couples and family
contexts. The areas of affective communication and conflict resolution are
almost identical in conceptualization, behavioral criteria and importance in
the spouse–spouse and par-ent–child communication domains. However, three other
rather sharply defined constructs in the parent–child literature are not fully
represented in the spouse–spouse literature: communication deviance (CD),
emotional overinvolvement and coercive process. In the cognitive realm, the CD
construct (unclear, amorphous, or fragmented communication) has been
investigated primarily among schizophrenic patients and their parents;
comparable work has not been done with couples. The more general construct of
communication has been explored with marital couples, with no theoretical link
to thought disorder and schizophrenia.
Coercive processes – the shaping of the behavior of parents by negative behavior on the part of the child – is similar to nega-tive escalation in couples. Although not yet investigated in cou-ples, it is quite conceivable that one spouse could effectively uti-lize a coercive process with the other spouse. Overinvolvement, which has been explored in the parent–child literature, may have a related domain in the marital literature, specifically, structure. Indeed, the over involvement construct has been seen as most relevant with children and parents and has little predictive utility in adult couple samples. However, it seems that the concept of structure, with the issues of leadership, dominance and submis-sion, and distribution of functions, is an area that needs further exploration in reference to both couples and the entire family.
Structure
For a
marriage or family to function as a unit requires leadership and distribution
of functions. Leadership, dominance and power distribution can all have a
profound effect on the quality of inter-action satisfaction and on adequate
functioning of both couples and families, both in ordinary and in stressful
circumstances.
Couples
Dominance
as measured by verbal frequency has not distin-guished functional and
dysfunctional families. When one spouse is depressed, the power distribution is
not always as theoretically hypothesized (i.e., depressed spouse submissive to
dominance of the nondepressed partner). Contrary to expectation, depressed
patients produce substantial control-oriented communication with their spouses
during an acute depressed episode. Introversion and interpersonal dependency
may reflect enduring abnormalities in the functioning of individuals with
remitted depression.
Families
Some
parent–offspring relationships are marked by unclear boundaries and
overdependence, often inhibiting the offspring’s ability to separate,
individuate, or recover from illness. With re-spect to psychiatric and
sometimes medical disorders, it is not unusual to see a pairing of an
overprotective, overinvolved parent with a highly disabled, passive, withdrawn
offspring. Because ill offspring in these families often elicit such responses,
an overin-volved relationship is best thought of as a dyadic attribute rather
than a problem generated by a parent. Overinvolvement is often difficult to
define or assess in parents of school-age or adoles-cent children. However,
among studies of youth, those focusing on separation anxiety, and school
refusal in particular, describe parental overinvolvement and protectiveness as
complicating features.
The term expressed emotion (EE) is used to refer
to criti-cal comments, hostility, and/or overinvolvement as expressed by a
family member toward another family member with a mental disorder. Studies
suggest that overinvolvement is a risk factor for later episodes of psychosis
among patients diagnosed with schizophrenia, independent of the level of
criticism demonstrated by the family.
Communication of Information
Verbal
communication between two or more individuals in-volves the various aspects of
information exchange, including the amount and clarity of the information and
the reception of the information by another. This broad concept of communica-tion
implies the willingness to convey information, the accuracy and clarity of the
information, and the accurate decoding of the information by the other.
Couples
The
amount and quality of verbal communication have differen-tiated distressed and
nondistressed couples, and treatment leads to an improvement in communication.
Five
areas of cognitive phenomena are hypothesized to play important roles in
marital communication and maladjust-ment: selective attention, attributions,
expectancies, assump-tions and standards. Not all of these areas have been
equally investigated.
Distressed
spouses focus on negative behavior; positive interactions often are ignored.
Distressed spouses tend to attribute their partner’s undesired communication
behavior as global and the partner is blamed for her or his negative behavior,
which is seen as intentional, global, stable and originating from internal
factors. In contrast, nondistressed individuals give each other credit for
positive behavior and overlook or exonerate their spouses for negative
behavior. While the evolution or developmental history of these cognitive sets
has not been clearly delineated, current evidence suggests that negative
attributions for partner behavior may predict marital satisfaction over time.
Families
Many of
the same disordered processes (e.g., expression of hos-tility or excessive
criticism, poor information exchange, lack of conflict resolution) in the
spousal communication literature are presumed to disrupt healthy family
functioning. Unlike in the marital literature, however, the independent
variable in family studies is often the presence or absence of a
psychopathologic condition in an offspring or parent rather than high or low
levels of marital distress.
Related Topics