Chapter: Medical Physiology: Female Physiology Before Pregnancy and Female Hormones
Regulation of the Female Monthly Rhythm-Interplay Between the Ovarian and Hypothalamic-Pituitary Hormones
Regulation of the Female Monthly Rhythm-Interplay Between the Ovarian and Hypothalamic-Pituitary Hormones
Now that we have presented the major cyclical changes that occur during the monthly female sexual cycle, we can attempt to explain the basic rhythmical mechanism that causes the cyclical variations.The Hypothalamus Secretes GnRH, Which Causes the Anterior Pituitary Gland to Secrete LH and FSH
As pointed out, secretion of most of the anterior pituitary hormones is controlled by “releasing hormones” formed in the hypothalamus and then transported to the anterior pituitary gland by way of the hypothalamic-hypophysial portal system. In the case of the gonadotropins, one releasing hormone, GnRH, is important. This hormone has been purifiedand has been found to be a decapeptide with the following formula:
Glu-His-Trp-Ser-Tyr-Gly-Leu-Arg-Pro-Gly-NH2
Intermittent, Pulsatile Secretion of GnRH by the Hypothalamus Stimulates Pulsatile Release of LH from the Anterior Pituitary Gland. Experiments have demonstrated that the hypo-thalamus does not secrete GnRH continuously but instead secretes it in pulses lasting 5 to 25 minutes that occur every 1 to 2 hours. The lower curve in Figure 81–8 shows the electrical pulsatile signals in the hypo-thalamus that cause the hypothalamic pulsatile output of GnRH.
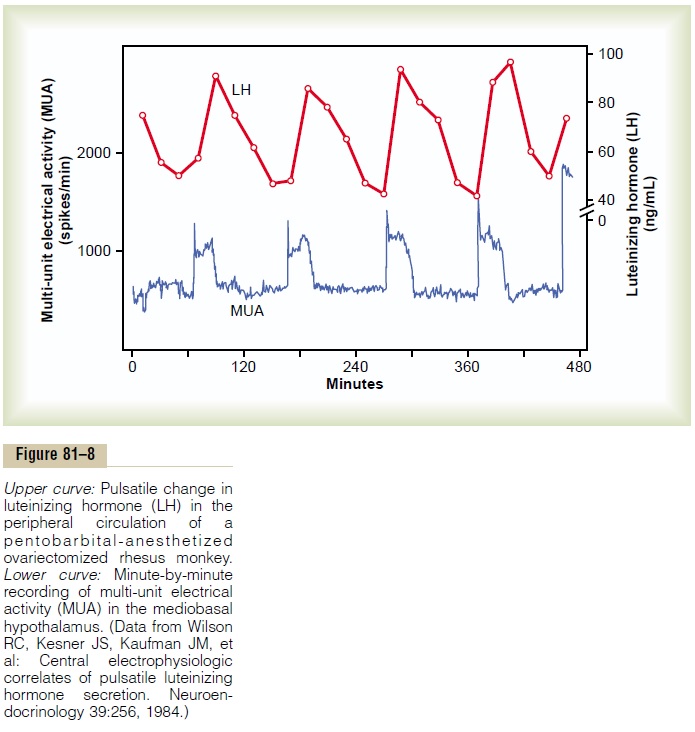
It is intriguing that when GnRH is infused continu-ously so that it is available all the time rather than in pulses, its ability to cause the release of LH and FSH by the anterior pituitary gland is lost. Therefore, for reasons unknown, the pulsatile nature of GnRH release is essential to its function.
The pulsatile release of GnRH also causes intermit-tent output of LH secretion about every 90 minutes. This is shown by the upper curve in Figure 81–8.
Hypothalamic Centers for Release of GnRH. The neuronalactivity that causes pulsatile release of GnRH occurs primarily in the mediobasal hypothalamus, especially in the arcuate nuclei of this area. Therefore, it is believed that these arcuate nuclei control most female sexual activity, although neurons located in the preoptic area of the anterior hypothalamus also secrete GnRH in moderate amounts. Multiple neu-ronal centers in the higher brain’s “limbic” system (the system for psychic control) transmit signals into the arcuate nuclei to modify both the intensity of GnRH release and the frequency of the pulses, thus providing a partial explanation of why psychic factors often modify female sexual function.
Negative Feedback Effects of Estrogen and Progesterone in Decreasing Both LH and FSH Secretion
Estrogen in small amounts has a strong effect to inhibit the production of both LH and FSH. Also, when progesterone is available, the inhibitory effect of estrogen is multiplied, even though progesterone by itself has little effect.
These feedback effects seem to operate mainly on the anterior pituitary gland directly, but they also operate to a lesser extent on the hypothalamus to decrease secretion of GnRH, especially by altering the frequency of the GnRH pulses.
Hormone Inhibin from the Corpus Luteum Inhibits FSH and LH Secretion. In addition to the feedback effects of estro-gen and progesterone, other hormones seem to be involved, especially inhibin, which is secreted along with the steroid sex hormones by the granulosa cells of the ovarian corpus luteum in the same way that Sertoli cells secrete inhibin in the male testes. This hormone has the same effect in the female as in the male—inhibiting the secretion of FSH and, to a lesser extent, LH by the anterior pituitary gland. Therefore, it is believed that inhibin might be especially impor-tant in causing the decrease in secretion of FSH and LH at the end of the monthly female sexual cycle.
Positive Feedback Effect of Estrogen Before Ovulation—The Preovulatory LH Surge
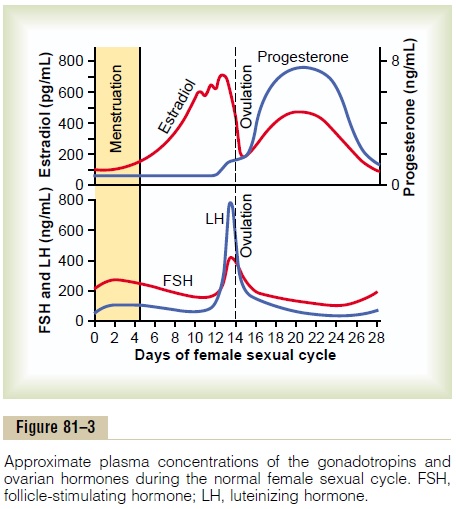
For reasons not completely understood, the anterior pituitary gland secretes greatly increased amounts of LH for 1 to 2 days beginning 24 to 48 hours before ovulation. This effect is demonstrated in Figure 81–3. The figure shows a much smaller preovulatory surge of FSH as well.
Experiments have shown that infusion of estrogen into a female above a critical rate for 2 to 3 days during the latter part of the first half of the ovarian cycle will cause rapidly accelerating growth of the ovarian folli-cles, as well as rapidly accelerating secretion of ovarian estrogens. During this period, secretions of both FSH and LH by the anterior pituitary gland are at first slightly suppressed. Then secretion of LH increases abruptly sixfold to eightfold, and secretion of FSH increases about twofold. The greatly increased secre-tion of LH causes ovulation to occur.
The cause of this abrupt surge in LH secretion is not known. However, several possible explanations are as follows: (1) It has been suggested that estrogen at this point in the cycle has a peculiar positive feedback effect of stimulating pituitary secretion of LH and, to a lesser extent, FSH; this is in sharp contrast to its normal neg-ative feedback effect that occurs during the remainder of the female monthly cycle. (2) The granulosa cells of the follicles begin to secrete small but increasing quan-tities of progesterone a day or so before the preovu-latory LH surge, and it has been suggested that this might be the factor that stimulates the excess LH secretion.
Without this normal preovulatory surge of LH, ovulation will not occur.
Feedback Oscillation of the Hypothalamic-Pituitary-Ovarian System
Now, after discussing much of the known information about the interrelations of the different components of the female hormonal system, we can attempt to explain the feedback oscillation that controls the rhythm of the female sexual cycle. It seems to operate in approximately the following sequence of three events.
1. Postovulatory Secretion of the Ovarian Hormones, and Depression of the Pituitary Gonadotropins. The easiest partof the cycle to explain is the events that occur during the postovulatory phase—between ovulation and the beginning of menstruation. During this time, the corpus luteum secretes large quantities of both prog-esterone and estrogen, as well as the hormone inhibin. All these hormones together have a combined nega-tive feedback effect on the anterior pituitary gland and hypothalamus, causing the suppression of both FSH and LH secretion and decreasing them to their lowest levels about 3 to 4 days before the onset of menstrua-tion. These effects are shown in Figure 81–3.
2. Follicular Growth Phase. Two to 3 days before men-struation, the corpus luteum has regressed to almost total involution, and the secretion of estrogen, proges-terone, and inhibin from the corpus luteum decreases to a low ebb. This releases the hypothalamus and anterior pituitary from the negative feedback effect of these hormones. Therefore, a day or so later, at about the time that menstruation begins, pituitary secretion of FSH begins to increase again, as much as twofold; then, several days after menstruation begins, LH secre-tion increases slightly as well. These hormones initiate new ovarian follicle growth and a progressive increase in the secretion of estrogen, reaching a peak estrogen secretion at about 12.5 to 13 days after the onset of the new female monthly sexual cycle.
During the first 11 to 12 days of this follicle growth, the rates of pituitary secretion of the gonadotropins FSH and LH decrease slightly because of the negative feedback effect, mainly of estrogen, on the anterior pituitary gland. Then there is a sudden, marked increase in the secretion of LH and, to a lesser extent, FSH. This is the preovulatory surge of LH and FSH, which is followed by ovulation.
3. Preovulatory Surge of LH and FSH Causes Ovulation. Atabout 11.5 to 12 days after the onset of the monthly cycle, the decline in secretion of FSH and LH comes to an abrupt halt. It is believed that the high level of estrogens at this time (or the beginning of proges-terone secretion by the follicles) causes a positive feedback stimulatory effect on the anterior pituitary, as explained earlier, which leads to a terrific surge in the secretion of LH and, to a lesser extent, FSH. What-ever the cause of this preovulatory LH and FSH surge, the great excess of LH leads to both ovulation and sub-sequent development of and secretion by the corpus luteum. Thus, the hormonal system begins its new round of secretions until the next ovulation.
Anovulatory Cycles—Sexual Cycles at Puberty
If the preovulatory surge of LH is not of sufficient magnitude, ovulation will not occur, and the cycle is said to be “anovulatory.”The phases of the sexual cycle continue, but they are altered in the following ways: First, lack of ovulation causes failure of development of the corpus luteum, so there is almost no secretion of progesterone during the latter portion of the cycle. Second, the cycle is shortened by several days, but the rhythm continues. Therefore, it is likely that proges-terone is not required for maintenance of the cycle itself, although it can alter its rhythm.
The first few cycles after the onset of puberty are usually anovulatory, as are the cycles occurring several months to years before menopause, presumably because the LH surge is not potent enough at these times to cause ovulation.
Puberty and Menarche
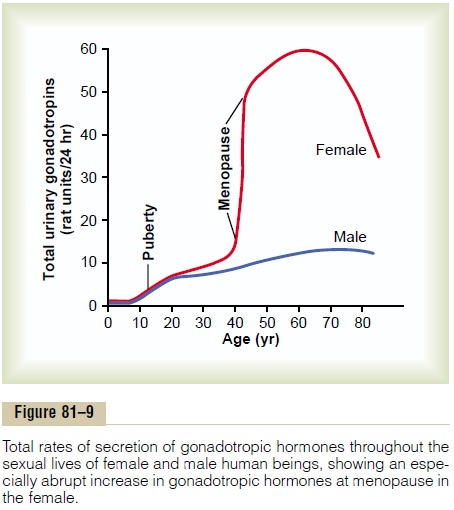
Puberty means the onset of adult sexual life, and menarche means the beginning of the cycle of menstruation. The period of puberty is caused by a gradual increase in gonadotropic hormone secretion by the pituitary, beginning in about the eighth year of life, as shown in Figure 81–9, and usually culminating in the onset of puberty and menstruation between ages 11 and 16 years in girls (average, 13 years).
In the female, as in the male, the infantile pituitary gland and ovaries are capable of full function if appro-priately stimulated. However, as is also true in the male, and for reasons not understood, the hypothala-mus does not secrete significant quantities of GnRH during childhood. Experiments have shown that the hypothalamus itself is capable of secreting this hormone, but the appropriate signal from some other area of brain to cause the secretion is lacking. There-fore, it is now believed that the onset of puberty is initiated by some maturation process that occurs else-where in the brain, perhaps somewhere in the limbic system.
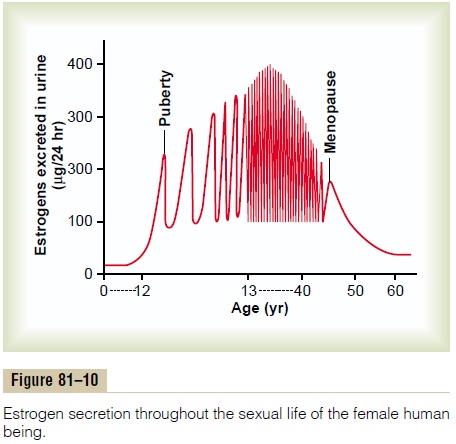
Figure 81–10 shows (1) the increasing levels of estro-gen secretion at puberty, (2) the cyclical variation during the monthly sexual cycle, (3) the further increase in estrogen secretion during the first few years of reproductive life, (4) the progressive decrease in estrogen secretion toward the end of reproductive life, and, finally, (5) almost no estrogen or progesterone secretion beyond menopause.
Menopause
At age 40 to 50 years, the sexual cycle usually becomes irregular, and ovulation often fails to occur.After a few months to a few years, the cycle ceases altogether, as shown in Figure 81–10. The period during which the cycle ceases and the female sex hormones diminish to almost none is called menopause.
The cause of menopause is “burning out” of the ovaries. Throughout a woman’s reproductive life, about 400 of the primordial follicles grow into mature follicles and ovulate, and hundreds of thousands of ova degenerate. At about age 45 years, only a few primor-dial follicles remain to be stimulated by FSH and LH, and, as shown in Figure 81–10, the production of estrogens by the ovaries decreases as the number of primordial follicles approaches zero. When estrogen production falls below a critical value, the estrogens can no longer inhibit the production of the gonadotropins FSH and LH. Instead, as shown in Figure 81–9, the gonadotropins FSH and LH (mainly FSH) are produced after menopause in large and con-tinuous quantities, but as the remaining primordial fol-licles become atretic, the production of estrogens by the ovaries falls virtually to zero.
At the time of menopause, a woman must readjust her life from one that has been physiologically stimu-lated by estrogen and progesterone production to one devoid of these hormones. The loss of estrogens often causes marked physiological changes in the function of the body, including (1) “hot flushes” characterized by extreme flushing of the skin, (2) psychic sensations of dyspnea, (3) irritability, (4) fatigue, (5) anxiety, (6) occasionally various psychotic states, and (7) decreased strength and calcification of bones through-out the body. These symptoms are of sufficient magni-tude in about 15 per cent of women to warrant treatment. If counseling fails, daily administration of estrogen in small quantities usually reverses the symp-toms, and by gradually decreasing the dose, post-menopausal women can likely avoid severe symptoms.
Related Topics