Chapter: Medical Physiology: Fetal and Neonatal Physiology
Onset of Breathing - Adjustments of the Infant to Extrauterine Life
Onset of Breathing
The most obvious effect of birth on the baby is loss of the placental connection with the mother and, there-fore, loss of this means of metabolic support. One of the most important immediate adjustments required of the infant is to begin breathing.
Cause of Breathing at Birth. After normal delivery from amother who has not been depressed by anesthetics, the child ordinarily begins to breathe within seconds and has a normal respiratory rhythm within less than 1 minute after birth. The promptness with which the fetus begins to breathe indicates that breathing is initiated by sudden exposure to the exterior world, probably result-ing from (1) a slightly asphyxiated state incident to the birth process, but also from (2) sensory impulses that originate in the suddenly cooled skin. In an infant who does not breathe immediately, the body becomes progressively more hypoxic and hypercapnic, which provides additional stimulus to the respiratory center and usually causes breathing within an additional minute after birth.
Delayed or Abnormal Breathing at Birth—Danger of Hypoxia. Ifthe mother has been depressed by a general anesthetic during delivery, which at least partially anesthetizes the fetus as well, the onset of respiration is likely to be delayed for several minutes, thus demonstrating the importance of using as little anesthesia as feasible. Also, many infants who have had head trauma during deliv-ery or who undergo prolonged delivery are slow to breathe or sometimes do not breathe at all. This can result from two possible effects: First, in a few infants, intracranial hemorrhage or brain contusion causes a concussion syndrome with a greatly depressed respira-tory center. Second, and probably much more impor-tant, prolonged fetal hypoxia during delivery can cause serious depression of the respiratory center.
Hypoxia frequently occurs during delivery because of (1) compression of the umbilical cord; (2) premature separation of the placenta; (3) excessive contraction of the uterus, which can cut off the mother’s blood flow to the placenta; or (4) excessive anesthesia of the mother, which depresses oxygenation even of her blood.
Degree of Hypoxia That an Infant Can Tolerate. In an adult,failure to breathe for only 4 minutes often causes death, but a neonate often survives as long as 10 minutes of failure to breathe after birth. Permanent and very serious brain impairment often ensues if breathing is delayed more than 8 to 10 minutes. Indeed, actual lesions develop mainly in the thalamus, in the inferior colliculi, and in other brain stem areas, thus permanently affecting many of the motor functions of the body.
Expansion of the Lungs at Birth. At birth, the walls of thealveoli are at first collapsed because of the surface tension of the viscid fluid that fills them. More than 25 mm Hg of negative inspiratory pressure in the lungs is usually required to oppose the effects of this surface tension and to open the alveoli for the first time. But once the alveoli do open, further respiration can be effected with relatively weak respiratory movements. Fortunately, the first inspirations of the normal neonate are extremely powerful, usually capable of creating as much as 60 mm Hg negative pressure in the intrapleural space.
Figure 83–3 shows the tremendous negative intrapleural pressures required to open the lungs at the onset of breathing. At the top is shown the pres-sure-volume curve (“compliance” curve) for the first breath after birth. Observe, first, the lower part of the curvebeginning at the zero pressure point and moving to the right. The curve shows that the volume of air in the lungs remains almost exactly zero until the negative pressure has reached -40 centimeters water (-30 mm Hg). Then, as the negative pressure increases to -60 centimeters of water, about 40 milliliters of air enters the lungs. To deflate the lungs, considerable pos-itive pressure, about +40 centimeters of water, is required because of viscous resistance offered by the fluid in the bronchioles.
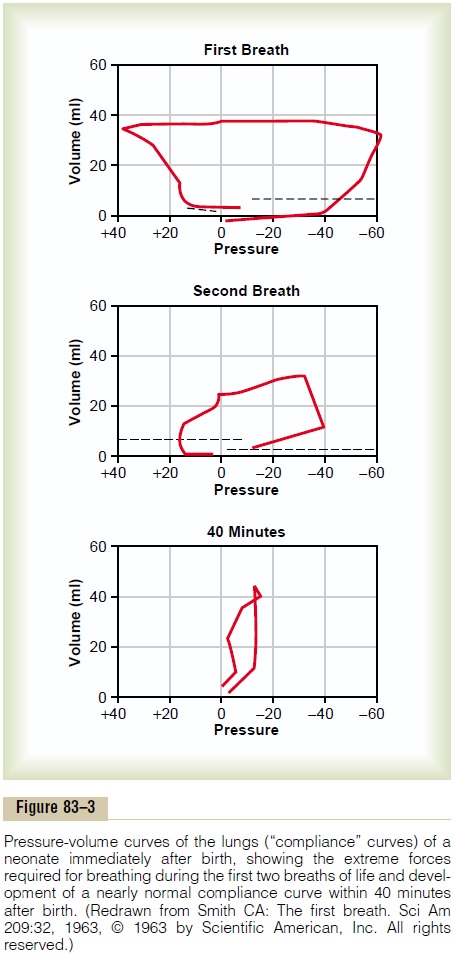
Note that the second breath is much easier, with far less negative and positive pressures required. Breathing does not become completely normal until about 40 minutes after birth, as shown by the third compliance curve, the shape of which compares favorably with that for the normal adult.
Respiratory Distress Syndrome Caused When Surfactant Secretion Is Deficient. A small number of infants, especially pre-mature infants and infants born of diabetic mothers, develop severe respiratory distress in the early hours to the first several days after birth, and some die within the next day or so. The alveoli of these infants at death contain large quantities of proteinaceous fluid, almost as if pure plasma had leaked out of the capillaries into the alveoli. The fluid also contains desquamated alveo-lar epithelial cells. This condition is called hyaline mem-brane disease because microscopic slides of the lungshow the material filling the alveoli to look like a hyaline membrane.
One of the most characteristic findings in respiratory distress syndrome is failure of the respiratory epithe-lium to secrete adequate quantities of surfactant, a sub-stance normally secreted into the alveoli that decreases the surface tension of the alveolar fluid, therefore allow-ing the alveoli to open easily during inspiration. The sur-factant-secreting cells (type II alveolar epithelial cells) do not begin to secrete surfactant until the last 1 to 3 months of gestation. Therefore, many premature babies and a few full-term babies are born without the capa-bility to secrete sufficient surfactant, which causes both a collapse tendency of the alveoli and development of pulmonary edema.
Related Topics