Chapter: Essentials of Psychiatry: Mood Disorders: Premenstrual Dysphoric Disorder
Mood Disorders: Premenstrual Dysphoric Disorder
Mood Disorders: Premenstrual Dysphoric Disorder
Definition
Premenstrual syndrome (PMS) is a combination of emotional, be-havioral
and physical symptoms that occur in the premenstrual or luteal phase of the
menstrual cycle. The term “premenstrual ten-sion” appeared in the medical
literature 70 years ago but widely accepted diagnostic criteria for PMS do not
exist. Approximately 80% of women report at least mild premenstrual symptoms,
20 to 50% report moderate to severe premenstrual symptoms, and approximately 5%
of women report severe symptoms for several days with impairment of role and
social functioning. The 5% of women with the severest form of PMS generally
have symptoms that meet the diagnostic criteria for premenstrual dysphoric
dis-order (PMDD).
The diagnostic criteria for PMDD are listed in the ap-pendix of DSM-IV
(American Psychiatric Association, 1994). A clinician can indicate that a woman
has symptoms that meet the diagnostic criteria for PMDD by using the DSM-IV
diagno-sis 311, depressive disorder not otherwise specified. To meet the PMDD
criteria, at least five out of 11 possible symptoms must be present in the
premenstrual phase; these symptoms should be absent shortly following the onset
of menses; and at least one of the five symptoms must be depressed mood,
anxiety, lability, or irritability. The PMDD criteria require that role
functioning be impaired as a result of the premenstrual symptoms. The
func-tional impairment reported by women with PMDD is similar in severity to
the impairment reported in major depressive disorder and dysthymic disorder (Pearlstein
et al., 2000). Unlike the func-tional
impairment reported in depressive disorders, women with severe PMS and PMDD
report more disruption in their relation-ships and parenting roles than in
their work roles.
The PMDD criteria require that a woman prospectively rate her emotional,
behavioral and physical symptoms over two men-strual cycles to confirm the
diagnosis. Charting two menstrual cycles is advantageous, since some women have
variability of symptom severity from cycle to cycle due to factors such as
sea-sonal worsening, or a woman might have the unusual presence of follicular
phase psychological symptoms due to a transient stres-sor. Recent studies tend
to utilize visual analog scales, or Likert scale daily rating forms such as the
Daily Record of Severity of Problems (Endicott and Harrison, 1990), with a
scoring method that compares the average of symptom scores during the
premen-strual days to the average of symptom scores postmenses.
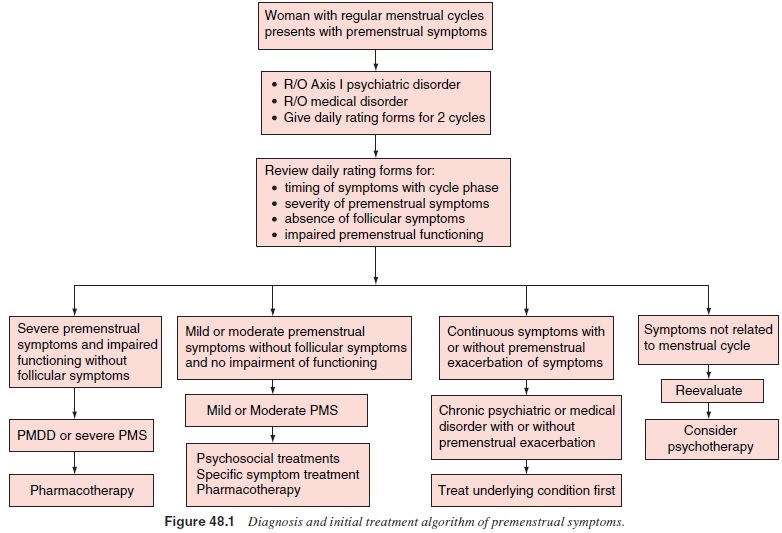
A woman presenting with PMS should ideally bring to her clinician two
cycles of an established daily rating form, oralternatively ratings of her most
problematic symptoms, rated with anchor points ranging from “not present” to
“severe”. The clinician should review the daily ratings to confirm that the
symptoms are in fact confined largely to the premenstrual phase, with the
relative absence of symptoms in the follicular phase, and the clinician should
also assess premenstrual functional impairment (Figure 48.1). Ratings that
demonstrate follicular symptoms with increased symptom severity in the
premenstrual phase suggest “premenstrual exacerbation” of an underlying
disorder rather than PMDD. The DSM-IV-TR PMDD criteria state
that the premenstrual symptoms should not be an exacerbation of an
underlying disorder, but that PMDD could be superimposed on another disorder,
like panic disorder. No formal guidelines exist for how to apply this criterion
clinically.
Related Topics