Chapter: Microbiology and Immunology: Bacteriology: Mycobacterium tuberculosis
Epidemiology - Mycobacterium tuberculosis
Epidemiology
Tuberculosis is the number one infectious killer disease worldwide.
◗ Geographical distribution
One-third of the world population is infected with M. tuberculosis. Nearly, two-thirds of all cases of tuberculosis occur in the devel-oping countries including India, Pakistan, China, Bangladesh, Philippines, Indonesia, Thailand, and Congo. Nearly, 3 million people die of tuberculosis every year and nearly 2 billion people have latent tuberculosis.
Tuberculosis is a major health problem in India. More than 40% of the population is infected with M. tuberculosis, and nearly 15 million people suffer from tuberculosis of which 3 million people are highly infectious open cases of tubercu-losis. Nearly half a million people die from the disease every year.
◗ Habitat
M. tuberculosis inhabits primarily the respiratory tract ofthe infected human host. The droplet nuclei consisting of M. tuberculosishave been found in the terminal air spaces of thelung.
Reservoir, source, and transmission of infection
Human beings are the only source and reservoir for M. tuberculosis infection. The infectiousness of the source is ofprimary importance, which determines the possibility of trans-mission of the disease. This depends on bacillary load of lesions and also on the morphology of the lesion. Lesions with cavities have 100–10,000 bacilli; therefore, cases with cavitary lesions are potentially highly infectious. Cases treated with antituber-cular therapy are less infectious than those who are not treated with any antitubercular drugs. The decrease in infectiousness is primarily due to reduction in the bacillary load in the lungs. Humans acquire M. tuberculosisinfection most frequently by inhalation of infectious aerosolized droplets. These infective droplets are usually coughed or sneezed into environment by a patient suffering from pulmonary tuberculosis. The acts of coughing, sneezing, and speaking release a large number of droplets containing as many as 3000 infectious airborne drop-let nuclei per cough. The droplet nucleus is small, measures 5 mm or less, and may contain approximately 1–10 tubercle bacilli. Theoretically, although a single tubercle bacillus may cause disease, in practice 5–200 inhaled bacilli are essential for infection. These droplets by virtue of their small size remain suspended in the air for a very long period of time. The infec-tion is acquired rarely by inoculation.
M. bovis infection is transmitted to humans by ingestionof raw milk of the cows infected with M. bovis. The infection among animals is spread by aerosolized bacilli in moist cough sprays. The infected animals usually excrete the bacilli in their milk. Person-to-person transmission of M. bovis usually does not occur.
Risk factors for tuberculosis: Primary infection of lungoccurs as a result of inhalation of the infectious aerosols. The risk of infection depends on the exposure to ultraviolet rays and ventilation; therefore the risk of infection is high in small rooms and in rooms with poor ventilation. There are many risk factors for tuberculosis:
· HIV is one of the most important risk factor. Case rates for individuals who are infected with both HIV and M. tuberculo-sisexceed the infective risk of individuals with M. tuberculosis infection who are not infected with HIV.
· Other factors that increase the risk of tuberculosis are ste-roid therapy, cancer chemotherapy, malignancies, and undernutrition. The latter condition alters CMI and, there-fore, is responsible for the increased frequency of tuberculo-sis in impoverished persons.
· Persons with certain human leukocytic antigen (HLA types) are at increased susceptibility to acquisition of tuberculosis. Hereditary factors, such as presence of a Bcg gene, also have a predisposition to tuberculosis.
· Nontubercular factors, such as pertussis, varicella, and mea-sles, may reactivate dormant and quiescent M. tuberculosis infection.
Infection in mammals: M. tuberculosisprimarily causes natu-ral infections in humans. The bacteria may also cause natural infections in other primates, dogs, and other animals, which come in close contact with infected humans. In experimental infections, M. tuberculosis is highly infectious for guinea pigs and hamsters but is usually nonpathogenic for bovines, goats, cats, and rabbits. Mice are moderately susceptible. M. bovis is more pathogenic for animals. The bacilli produce tuberculosis in cattle as well as in humans and other primates. Experimentally it is highly pathogenic for guinea pigs, calves, and rats and non-pathogenic for fowl.
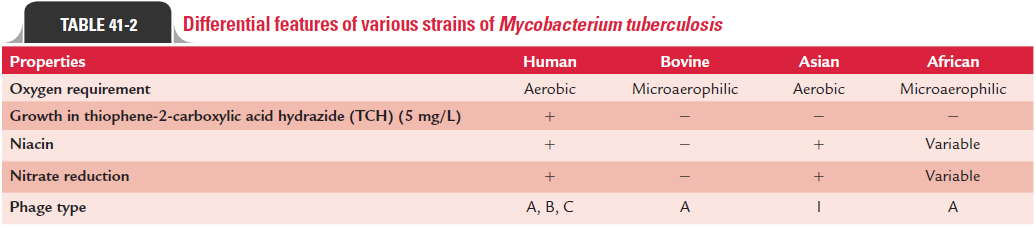
African strains or M. africanum are the strains of tubercle bacilli that are isolated mostly from Africa. Asian type strains are of low virulence for guinea pigs, susceptible to hydro-gen peroxide, resistant to INH, and are usually isolated from South India. These Asian strains have also been isolated from other Asian countries and from Asians abroad. Differential features of various strains of M. tuberculosis are summarized in Table 41-2.
Related Topics