Chapter: Medical Physiology: Somatic Sensations: II. Pain, Headache, and Thermal Sensations
Dual Pathways for Transmission of Pain Signals into the Central Nervous System
Dual Pathways for Transmission of Pain Signals into the Central Nervous System
Even though all pain receptors are free nerve endings, these endings use two separate pathways for transmit-ting pain signals into the central nervous system. The two pathways mainly correspond to the two types of pain—a fast-sharp pain pathway and a slow-chronicpain pathway.
Peripheral Pain Fibers—“Fast” and “Slow” Fibers. The fast-sharp pain signals are elicited by either mechanical or thermal pain stimuli; they are transmitted in the peripheral nerves to the spinal cord by small type Ad fibers at velocities between 6 and 30 m/sec. Conversely, the slow-chronic type of pain is elicited mostly by chemical types of pain stimuli but sometimes by persisting mechanical or thermal stimuli. This slow-chronic pain is transmitted to the spinal cord by type C fibers at velocities between 0.5 and 2 m/sec.
Because of this double system of pain innervation, a sudden painful stimulus often gives a “double” pain sensation: a fast-sharp pain that is transmitted to the brain by the Ad fiber pathway, followed a second or so later by a slow pain that is transmitted by the C fiber pathway. The sharp pain apprises the person rapidly of a damaging influence and, therefore, plays an impor-tant role in making the person react immediately to remove himself or herself from the stimulus. The slow pain tends to become greater over time. This sensation eventually produces the intolerable suffering of long-continued pain and makes the person keep trying to relieve the cause of the pain.
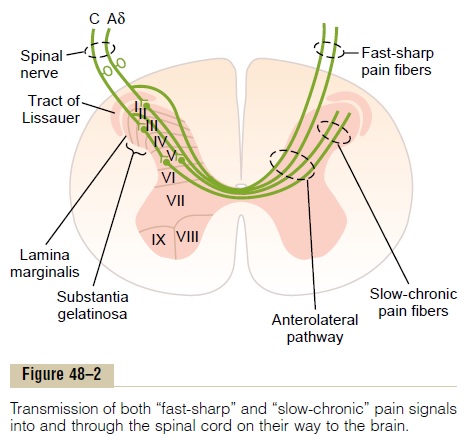
On entering the spinal cord from the dorsal spinal roots, the pain fibers terminate on relay neurons in the dorsal horns. Here again, there are two systems for processing the pain signals on their way to the brain, as shown in Figures 48–2 and 48–3.
Dual Pain Pathways in the Cord and Brain Stem—The Neospinothalamic Tract and the Paleospinothalamic Tract
On entering the spinal cord, the pain signals take two pathways to the brain, through (1) the neospinothala-mic tract and (2) the paleospinothalamic tract.
Neospinothalamic Tract for Fast Pain. The fast type Adpain fibers transmit mainly mechanical and acute thermal pain. They terminate mainly in lamina I (lamina marginalis) of the dorsal horns, as shown in Figure 48–2, and there excite second-order neurons of the neospinothalamic tract. These give rise to long fibers that cross immediately to the opposite side of the cord through the anterior commissure and then turn upward, passing to the brain in the anterolateral columns.
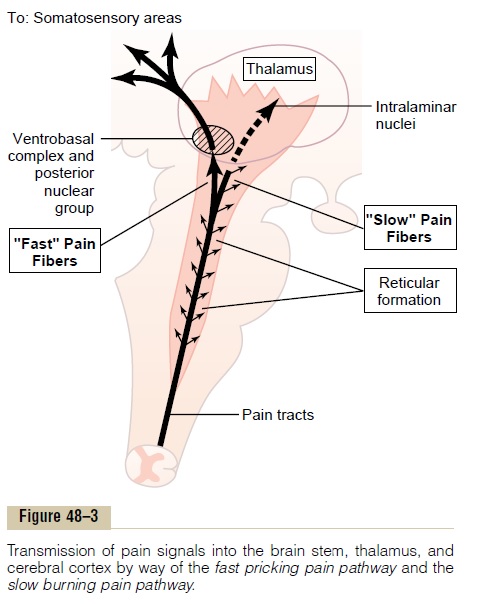
Termination of the Neospinothalamic Tract in the Brain Stem and Thalamus. A few fibers of the neospinothal-amic tract terminate in the reticular areas of the brain stem, but most pass all the way to the thalamus without interruption, terminating in the ventrobasal complex along with the dorsal column–medial lemniscal tract for tactile sensations.
A few fibers also terminate in the posterior nuclear group of the thalamus. From these thalamic areas, the signals are transmitted to other basal areas of the brain as well as to the somatosensory cortex.
Capability of the Nervous System to Localize Fast Pain in the Body. The fast-sharp type of pain can be local-ized much more exactly in the different parts of the body than can slow-chronic pain. However, when only pain receptors are stimulated, without the simultane-ous stimulation of tactile receptors, even fast pain may be poorly localized, often only within 10 centimeters or so of the stimulated area. Yet when tactile receptors that excite the dorsal column–medial lemniscal system are simultaneously stimulated, the localization can be nearly exact.
Glutamate, the Probable Neurotransmitter of the Type Ad Fast Pain Fibers. It is believed thatglutamateis theneurotransmitter substance secreted in the spinal cord at the type Ad pain nerve fiber endings. This is one of the most widely used excitatory transmitters in the central nervous system, usually having a duration of action lasting for only a few milliseconds.
Paleospinothalamic Pathway for Transmitting Slow-Chronic Pain. The paleospinothalamic pathway is a much oldersystem and transmits pain mainly from the peripheral slow-chronic type C pain fibers, although it does trans-mit some signals from type Ad fibers as well. In this pathway, the peripheral fibers terminate in the spinal cord almost entirely in laminae II and III of the dorsal horns, which together are called the substantia gelati-nosa, as shown by the lateral most dorsal root type Cfiber in Figure 48–2. Most of the signals then pass through one or more additional short fiber neurons within the dorsal horns themselves before entering mainly lamina V, also in the dorsal horn. Here the last neurons in the series give rise to long axons that mostly join the fibers from the fast pain pathway, passing first through the anterior commissure to the opposite side of the cord, then upward to the brain in the anterolat-eral pathway.
Substance P, the Probable Slow-Chronic Neurotrans- mitter of Type C Nerve Endings. Research experi-ments suggest that type C pain fiber terminals entering the spinal cord secrete both glutamate transmitter and substance P transmitter. The glutamate transmitter acts instantaneously and lasts for only a few millisec-onds. Substance P is released much more slowly, build-ing up in concentration over a period of seconds or even minutes. In fact, it has been suggested that the “double” pain sensation one feels after a pinprick might result partly from the fact that the glutamate transmitter gives a faster pain sensation, whereas the substance P transmitter gives a more lagging sensa-tion. Regardless of the yet unknown details, it seems clear that glutamate is the neurotransmitter most involved in transmitting fast pain into the central nervous system, and substance P is concerned with slow-chronic pain.
Projection of the Paleospinothalamic Pathway (Slow-Chronic Pain Signals) into the Brain Stem and Thala- mus. The slow-chronic paleospinothalamic pathwayterminates widely in the brain stem, in the large shaded area shown in Figure 48–3. Only one tenth to one fourth of the fibers pass all the way to the thala-mus. Instead, most terminate in one of three areas: (1) the reticular nuclei of the medulla, pons, and mesen-cephalon; (2) the tectal area of the mesencephalon deep to the superior and inferior colliculi; or (3) theperiaqueductal gray region surrounding the aqueductof Sylvius. These lower regions of the brain appear to be important for feeling the suffering types of pain, because animals whose brains have been sectioned above the mesencephalon to block pain signals from reaching the cerebrum still evince undeniable evi-dence of suffering when any part of the body is trau-matized. From the brain stem pain areas, multiple short-fiber neurons relay the pain signals upward into the intralaminar and ventrolateral nuclei of the thala-mus and into certain portions of the hypothalamus and other basal regions of the brain.
Very Poor Capability of the Nervous System to Local-ize Precisely the Source of Pain Transmitted in the Slow-Chronic Pathway. Localization of pain transmit-ted by way of the paleospinothalamic pathway is poor. For instance, slow-chronic pain can usually be local-ized only to a major part of the body, such as to one arm or leg but not to a specific point on the arm or leg. This is in keeping with the multisynaptic, diffuse con-nectivity of this pathway. It explains why patients often have serious difficulty in localizing the source of some chronic types of pain.
Function of the Reticular Formation, Thalamus, and Cerebral Cortex in the Appreciation of Pain. Complete removal ofthe somatic sensory areas of the cerebral cortex does not destroy an animal’s ability to perceive pain. There-fore, it is likely that pain impulses entering the brain stem reticular formation, the thalamus, and other lower brain centers cause conscious perception of pain. This does not mean that the cerebral cortex has nothing to do with normal pain appreciation; electri-cal stimulation of cortical somatosensory areas does cause a human being to perceive mild pain from about 3 per cent of the points stimulated. However, it is believed that the cortex plays an especially important role in interpreting pain quality, even though pain per-ception might be principally the function of lower centers.
Special Capability of Pain Signals to Arouse Overall Brain Excitability. Electrical stimulation in thereticular areasof the brain stem and in the intralaminar nuclei of the thalamus, the areas where the slow-suffering type ofpain terminates, has a strong arousal effect on nervous activity throughout the entire brain. In fact, these two areas constitute part of the brain’s principal “arousal system,”.This explains why it is almost impossible for a person to sleep when he or she is in severe pain.
Surgical Interruption of Pain Pathways. When a person hassevere and intractable pain (sometimes resulting from rapidly spreading cancer), it is necessary to relieve the pain. To do this, the pain nervous pathways can be cut at any one of several points. If the pain is in the lower part of the body, a cordotomy in the thoracic region of the spinal cord often relieves the pain for a few weeks to a few months. To do this, the spinal cord on the side opposite to the pain is partially cut in its anterolateralquadrant to interrupt the anterolateral sensory pathway.
A cordotomy, however, is not always successful in relieving pain, for two reasons. First, many pain fibers from the upper part of the body do not cross to the opposite side of the spinal cord until they have reached the brain, so that the cordotomy does not transect these fibers. Second, pain frequently returns several months later, partly as a result of sensitization of other pathways that normally are too weak to be effectual (e.g., sparse pathways in the dorsolateral cord). Another experi-mental operative procedure to relieve pain has been to cauterize specific pain areas in the intralaminar nuclei in the thalamus, which often relieves suffering types of pain while leaving intact one’s appreciation of “acute” pain, an important protective mechanism.
Related Topics