Chapter: Microbiology and Immunology: Mycology, Fungi: Opportunistic Fungal Infections
Aspergillus Species
Aspergillus Species
Properties
Aspergillus species are molds.
· They have septate hyphae that form V-shaped dichotomous branches (Fig. 74-3). The Aspergillus species are identified by (a) their morphological features, (b) the pattern of conidio-phore development, and (c) the color of the conidia.
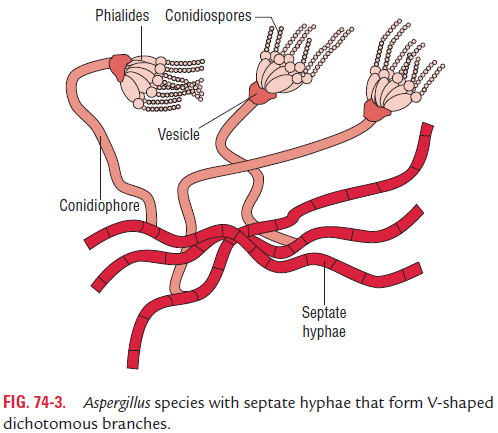
· The presence of septate hyphae that branch at 45° angles is the typical feature of Aspergillus species hyphae. The hyphae in tissues are best demonstrated with silver stains. The walls of the hyphae are more or less parallel, unlike those of Mucor and Rhizopus, which are more or less irregular.
· Lactophenol cotton blue (LPCB) preparation of the colo-nies shows septate hyphae and branching conidiophores. Asexual conidia arranged in chains are present on elongated cells known as sterigmata. The latter is present on the vesi-cle of the conidiophores. The conidia of Aspergillustypically form radiating chains in contrast to Rhizopus and Mucor, which are found within sporangia.
· The fungus grows rapidly on SDA and other culture media at 25°C. Aspergillus produces colonies within 1–2 days and shows a velvety surface.
Pathogenesis and Immunity
Aspergillus species rarely cause infections in immunocompe-tent individuals. They cause invasive infections mostly in the patients who are immunocompromised either due to (a) use of immunosuppressive drugs, (b) underlying lung diseases, or (c) immunodeficiency diseases, such as HIV. In immunocom-promised host, Aspergillus species cause invasion of the blood, thereby causing infarction, hemorrhage, and necrosis of lung tissues.Aspergillus spp. also produces toxic metabolites that inhibit macrophage and neutrophil phagocytosis, facilitating dissemination of the infection.
Aspergillus species unlike Candida species do not form the partof normal flora of humans. They are ubiquitous in the environ-ment; hence transmission of infection is mostly exogenous.
Clinical Syndromes
In immunocompetent hosts, Aspergillus species may primar-ily affect the lungs, causing four main syndromes including (a) allergic bronchopulmonary aspergillosis, (b) chronic necro-tizing aspergillus pneumonia, (c) aspergilloma, and (d) invasive aspergillosis.
Allergic bronchopulmonary aspergillosis: It is a hypersensi-tivity reaction to A. fumigatus organisms, which have colonized in tracheobronchial tree. This condition occurs often in asso-ciation with asthma and cystic fibrosis.
Chronic necrotizing pulmonary aspergillosis: It is asubacute infection seen in patients with some degree of immunosuppression. The condition occurs in conjunction with alcoholism, underlying lung disease, or chronic cortico-steroid therapy.
Aspergilloma: It is a condition that occurs in a preexist-ing cavity in the lung parenchyma. This cavity may have been caused earlier by tuberculosis, sarcoidosis, cystic fibrosis, and emphysematous bullae. The condition is characterized by the presence of a ball of fungus within the cavity. The fungus, however, does not invade the cavity. It may cause hemoptysis.
Invasive aspergillosis: It is a rapidly progressive infection inpatients who are severely immunocompromised. The condition is mostly fatal. In immunocompromised host, Aspergillus organ-isms cause a disseminated disease, leading to endophthalmitis, endocarditis, and abscesses in the viscera, such as liver, spleen, kidney, soft tissues, and bone.
Epidemiology
Various clinical manifestations of Aspergillus infection have been documented worldwide. The incidence of allergic bron-chopulmonary aspergillosis has been increasingly documented in people with asthma in United Kingdom. Aspergillus species unlike Candida species do not form the part of normal flora of humans. They are ubiquitous in the environment; hence trans-mission of infection is mostly exogenous.
Laboratory Diagnosis
Laboratory diagnosis of invasive aspergillosis or chronic nec-rotizing aspergillus pneumonia depends on demonstration of Aspergillus in tissue by direct microscopy and culture.
Treatment
Amphotericin B is most frequently used for treatment of inva-sive aspergillosis. However, the outcome of treatment is not sat-isfactory. Caspofungin is an alternative drug given to patients who do not respond to amphotericin B. Aspergilloma is treated best by removal of the fungus ball from the cavity by surgery.
Prevention and Control
There are no specific preventive measures available against aspergillosis.
Related Topics