Chapter: Surgical Pathology Dissection : The Endocrine System
Adrenal Glands : Surgical Pathology Dissection
Adrenal Glands
Adrenalectomies
Extrinsic
hormonal influences and intrinsic pathologic processes have profound and
predict-able effects on the size, color, and shape of the adrenal gland. For
example, the pathogenesis of hypercortisolism is frequently suggested by the
size and color of the adrenal cortex, and the distinction between benign and
potentially malignant cortical neoplasms is often based on the dimensions and
weight of the tumor. There-fore, careful examination of the gross specimen
plays an important role in recognizing and inter-preting pathologic processes
involving the adre-nal gland.
A
thorough evaluation of the specimen re-quires a certain familiarity with the
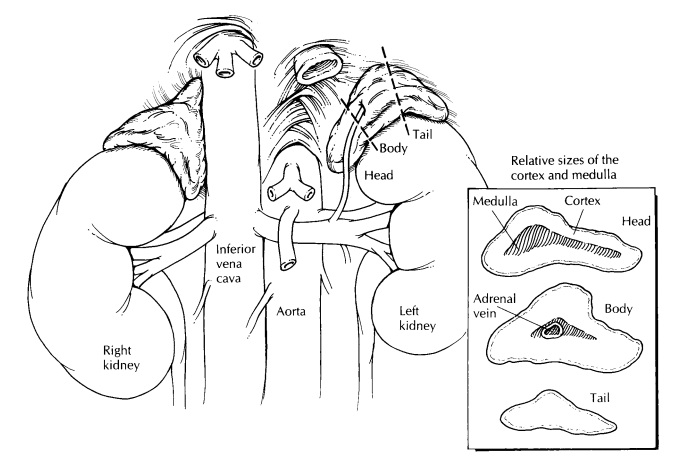
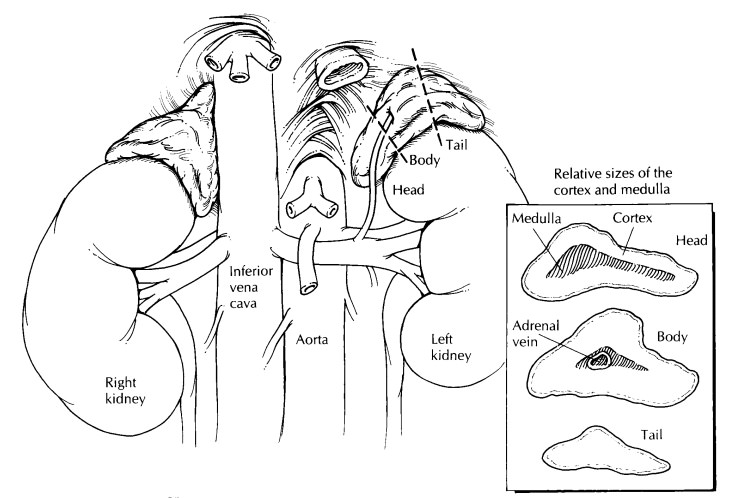
anatomy and weight of the normal adrenal gland. As illus-trated, the right
adrenal gland has the shape of a pyramid and the left adrenal gland the shape
of a crescent. The average weight of each is ap-proximately 4 g in the adult.
Weights of 6 g or more are abnormal. Specimen orientation is easily achieved by
locating the concave surface of the specimen. This concavity is the point at
which the adrenal abuts the ipsilateral kidney, and thus it represents the
inferolateral aspect of the speci-men. The adrenal gland is considered a
tripartite structure composed of a head, body, and tail. The head is the thickest
and broadest portion of the adrenal and is situated most medially. The middle
third represents the body. The thinnest and most lateral third represents the
tail. Unlike the kidney, blood does not enter the adrenal at a single vascular
pedicle. Instead, numerous small arteries pierce the cortex at multiple sites.
Most of these vessels are too small to appreciate grossly. In contrast, the
adrenal is drained by asingle vein. This vein exits the adrenal at the junction
of the body and the head of the gland and is usually visible to the naked eye,
especially when filled and distended by tumor.
Examine
the contours of the adrenal gland. Be sure to ink the soft tissues overlying
any areas where tumor bulges from the surface of the adre-nal, since these
areas represent soft tissue mar-gins. Look for and sample the adrenal vein. The
entire specimen should then be measured and weighed. Distinguishing between a
benign and malignant adrenal neoplasm is often done by weight. It is therefore
critical that you accu-rately weigh the intact fresh specimen before it is
fixed and before tissue is procured for additional studies. For tumors between
50 and 100 g we recommend that you carefully remove any extra-neous soft tissue
not near margins closely ap-proached by the tumor before weighing. If the gland
appears enlarged, determine and docu-ment whether this enlargement is due to a
solitary mass, multiple nodules, or diffuse hyperplasia. Extended resections of
primary adrenal tumors may also include portions of adjacent kidney, liver,
and/or abdominal wall. The presence and appearance of these structures should
be noted, and their relationships to the adrenal tumor should be described.
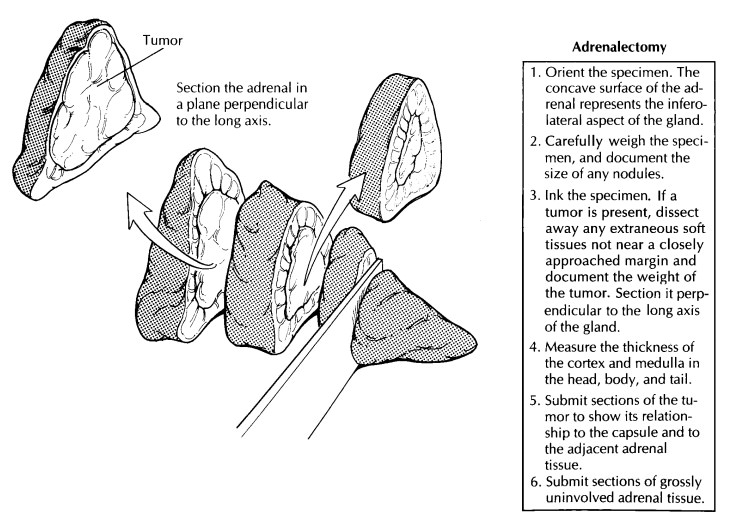
Unless otherwise indicated, the adrenal should always be sectioned in the transverse plane. This plane of sectioning optimizes evaluation of the relative sizes of the cortical and medullary com-partments. Serially section the adrenal gland at 2- to 3-mm intervals perpendicular to the long axis of the specimen. Keep in mind that al-though the adrenal gland is removed as a single structure, it is both structurally and function-ally compartmentalized into a steroid-secreting cortex and a chromaffin-positive medulla.
This compartmentalization will become most
appar-ent when the adrenal is sectioned. The medulla is seen as an inner gray
or white band confined mostly to the head of the adrenal. This central band is
sharply demarcated from the outer yellow-brown cortex. The inner zone of the
cortex is typically brown, while the outer zone of the cortex is often yellow.
The inner zone corres-ponds to the lipofuscin-laden zona reticularis and the
outer zone to the lipid-laden zona glomeru-losa and zona fasciculata. Measure
and record the thickness of these compartments at three levels— the head, body,
and tail. Remember to docu-ment the exact dimensions of any tumors and to
record the appearance of the tumor’s cut surface: What is its color? Is it
necrotic and/or hemor-rhagic? Is it encapsulated? Does it extend beyond the
adrenal and into adjacent tissues?
Before
the specimen is fixed in formalin, ask yourself if fresh tissue should be
specially pro-cessed. For example, adrenal cortical neoplasms are sometimes
evaluated for steroid content. Viable fresh tissue from these tumors can be
snap frozen in liquid nitrogen and stored in a 2708C
freezer for easy retrieval if tissue is laterneeded for biochemical analysis.
Fresh tissues from adrenal medullary neoplasms have histori-cally been
processed in dichromate fixatives (e.g., Zenker’s solution) to preserve
cytoplasmic chro-maffin granules. Today, this practice has limited value
because these same catecholamines can be more precisely characterized and
quantified from the patient’s serum. Perhaps the strongest indica-tion for
special tissue processing is if the tumor was resected from a young patient.
For adrenal tumors from pediatric patients—where a primi-tive neuroblastic
tumor is often suspected— fresh tissue should be set aside for cytogenetic,
molecular (e.g., N-myc amplification), and ultra-structural analysis.
Sections
from a tumor should be taken to de-monstrate the relationship of the tumor to
the adrenal, to the tumor capsule, and to any associ-ated soft tissues and
visceral organs. Do notforget to take sections from the surgical margins,
including an appropriate margin from all struc-tures represented in the
extended resection (e.g., abdominal wall, kidney) and from the per-iadrenal fat
overlying a bulging tumor. Large adrenal tumors should be sampled to include
all components contributing to its often variegated appearance on cut section.
For the uninvolved adrenal gland and for specimens that do not have a discrete
lesion, submit a representative section from the head, body, and tail. To best
demonstrate the cortex and medulla, these sec-tions should be taken
perpendicular to the long axis of the gland.![]()
Regional
lymph nodes will generally not be found in the specimen but may be separately
submitted by the surgeon. Any lymph nodes that are present should, of course,
be sampled for histologic evaluation.
Important Issues to Address in Your Surgical Pathology Report on Adrenalectomies
• What procedure was performed, and what
structures/organs are present?
• What are the dimensions and weight of the
adrenal gland?
• For focal tumors: From which compartment
(cortex or medulla) does the tumor appear to arise? What are the dimensions and
weight of the tumor? Is the tumor benign, malignant, or of uncertain malignant
potential? Does the tumor infiltrate vessels, the tumor capsule, and/ or the
surrounding tissues? What is the status of the surgical margins? Has the tumor
me-tastasized to regional lymph nodes? If so, how many lymph nodes were
removed, and how many are involved by tumor?
• For diffuse processes: Which compartment
(cortex or medulla) is expanded? Is the com-partment uniformly enlarged, or is
the enlarge-ment due to multiple nodules?
Related Topics