Chapter: Clinical Cases in Anesthesia : Abdominal Aortic Aneurysm
Which anesthetic techniques are appropriate for AAA surgery?
Which
anesthetic techniques are appropriate for AAA surgery?
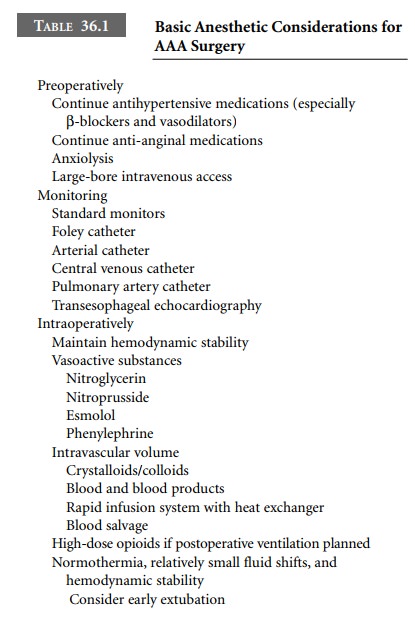
All antihypertensive and anti-anginal
medications should be continued until the time of surgery. Preoperative
sedation should be based on the patient’s clinical condition and concurrent
medical diseases. Some form of anxiolysis should be administered, as
hypertension and tachycardia may increase the risk of aneurysm leakage or
rupture, or induce myocardial ischemia in patients with concurrent coronary
artery disease. Patients presenting for aortic surgery may be very unstable
hemodynamically due to ongoing hemorrhage, myocardial ischemia, and/or
conges-tive heart failure. Organ malperfusion is also a major problem. It is,
therefore, recommended that patients who present for emergency aortic surgery
are intensely moni-tored in order to control blood pressure and resuscitate
appropriately.
In patients with aortic disease, the paramount
goal is the maintenance of hemodynamic stability, while provid-ing amnesia,
analgesia, and immobility. As the aorta remains at risk of rupture or extension
of the dissection, blood pressure must be strictly controlled. β-Adrenergic blockade and vasodilators are the mainstays for
minimiz-ing the driving force and the ejection velocity of blood, while
maintaining adequate perfusion pressure. At the other end of the spectrum are
patients who present in hypovolemic shock due to leaking or rupture of the
aorta. In this situation, maintaining volume status, securing the airway, and
immediate surgical control are the main goals.
All patients presenting for emergency aortic
surgery are considered to have a full stomach, while elective cases must be
considered individually. Avoidance of hemodynamic aberrations during induction
and tracheal intubation is desirable. Any number of anesthetic agents can
accomplish these goals and the choice is a personal decision that is dependent
on the clinical situation. High-dose opioid tech-niques are still commonly
employed for those patients in whom postoperative ventilatory support is
anticipated; however, normothermic, hemodynamically stable patients may be
considered for early extubation. Vasoactive medica-tions, such as
nitroprusside, nitroglycerin, and esmolol should be prepared preoperatively,
including diluted amounts for bolus administration (Table 36.1).
Related Topics