Chapter: Clinical Cases in Anesthesia : Abdominal Aortic Aneurysm
Explain the hemodynamic consequences of aortic cross-clamping
Explain
the hemodynamic consequences of aortic cross-clamping.
The most consistent hemodynamic response to
acute aortic occlusion is an abrupt increase in afterload with a resultant
increase in proximal aortic pressure. During supraceliac aortic occlusion,
there is an increase in preload due to volume redistribution from veins distal
to the site of aortic occlusion. The increases in afterload, preload, and
possibly contractility resulting from aortic occlusion may exacerbate
myocardial oxygen demand and possibly result in myocardial ischemia. Because of
the expected increases in preload from aortic occlusion, the pre-occlusion
preload should be maintained low. Venodilators such as nitroglyc-erin (NTG) may
be titrated in order to further decrease preload and arterial dilators may be
used to control increases in afterload. During aortic occlusion, attention
should be directed toward maintaining preload, which may be complicated by
continued blood loss.
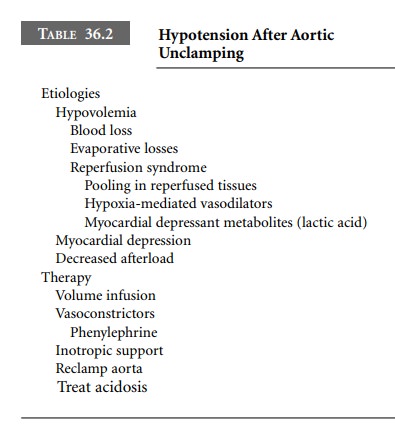
Intraoperative hypotension may result from
multiple causes. Hypovolemia, myocardial depression, and decreases in afterload
should be considered. Reperfusion is associated with hypotension. Hypotension
may be caused by central hypovolemia due to blood pooling in reperfused
tissues, hypoxia-mediated vasodilation, and accumulation of vasoac-tive or
myocardial-depressant metabolites, such as lactate. Treatment should be
directed toward rapid correction of hypovolemia, acidosis, and hypocalcemia, as
well as the judi-cious administration of vasoactive drugs. If there is
difficulty obtaining hemodynamic stability, the aorta can be temporar-ily
re-occluded while resuscitation continues (Table 36.2).
Renal insufficiency may occur as a result of
abdominal aortic reconstruction. It is possible that pharmacologic agents may
provide renal protection during repair. Although mannitol may result in greater
diuresis on post-operative day 1 and has less subclinical glomerular and renal
tubular damage, it most probably has no effect on postoperative blood urea
levels, serum creatinine concen-tration, or creatinine clearance. There is
little evidence of the effectiveness of furosemide as a renal protective agent.
Theoretically, the perioperative use of low
doses of dopamine may confer renal protection in high-risk individuals.
Low-dose dopamine (1–3 μg/kg/min) dilates renal afferent arterioles and
increases renal blood flow, independent of its cardiac effects. Dopamine
infusion during aortic clamping results in a significant rise in urine sodium
output, potassium output, creatinine clearance, and urine volume. The use of
perioperative dopamine during aortic surgery is associated with increases in
effective renal plasma flow and glomerular filtration rate as well as
fractional excre-tion of sodium during the postoperative period; however, no
studies have demonstrated a renal protective effect of low-dose dopamine. It is
most likely that renal-dose dopamine administration during the perioperative
period confers no advantage over the maintenance of euvolemia in most vascu-lar
patients during infrarenal AAA repair.
Visceral ischemia (which does not occur with
infrarenal aortic clamping) may initiate fibrinolysis. Antifibrinolytic agents
should be strongly considered if supraceliac occlusion is anticipated.
Aminocaproic acid, tranexamic acid, and aprotinin are all effective in
decreasing fibrinolytic activity.
Related Topics