Chapter: Surgical Pathology Dissection : Larynx
Total Laryngectomy
Total Laryngectomy
The
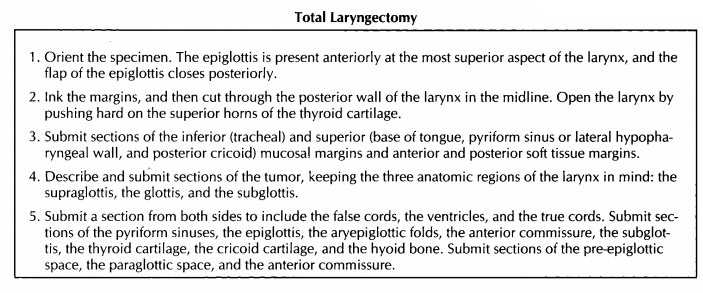
easiest way to orient a total laryngectomy specimen is to identify the
epiglottis. The epiglot-tis is present anteriorly at the most superior aspect
of the larynx, and the flap of the epiglottis closes posteriorly. If the
epiglottis is not present, then the thyroid cartilage can be used to orient the
specimen. The superior horns of the thyroid carti-lage are located superiorly
and project poste-riorly, while the V-shaped apex of the thyroid cartilage
points anteriorly.
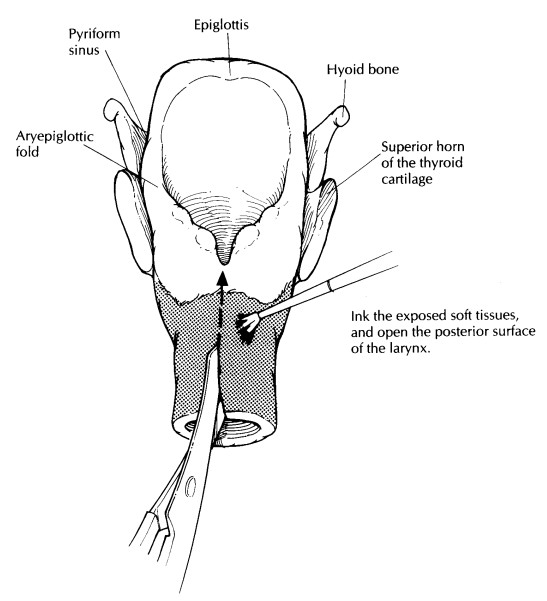
After
the specimen has been oriented, ink the soft tissue and mucosal margins. The
mucosal margins essentially form two rings. The inferior ring is formed by the
trachea, and the superior ring is formed by the circular opening of the larynx
into the pharynx. After the margins have been inked, cut through the posterior
wall of the larynx in the midline using a pair of scissors. This posterior
midline approach will fully expose the mucosal surfaces of the larynx without
disrupting the ana-tomic structures located along its anterior and internal
walls. The larynx can then be cracked open posteriorly by expanding the
posterior opening with your thumbs. The easiest and safest way to do this is to
push hard on the superior horns of the thyroid cartilage. The posterior aspect
of the larynx can then be kept open using a small wooden stick. The opened
larynx should be photographed to document the location and size of the tumor.
Depending on the preferences of your laboratory, the larynx can be processed
fresh or after fixation.
Continue
your dissection by sampling the mu-cosal margins. Sampling the inferior mucosal
margin is a relatively simple step. If this margin is not closely approached by
tumor, it can be taken as a single shave section of the tracheal stump. If the
tumor is close to the inferior margin, take perpendicular sections. Sampling
the supe-rior mucosal margin, on the other hand, is much more labor intensive.
This mucosal margin spans a number of important laryngeal structures, and great
care must be taken to sample the margin thoroughly and to designate each
sam-pled margin as precisely as possible. As illus-trated, the superior mucosal
margin is formed (1) anteriorly by the mucosa of the base of the tongue, (2)
laterally by the pyriform sinuses or lateral walls of the posterior
hypopharynx, and (3) posteriorly by the posterior cricoid mucosa. Perpendicular
sections of each of these three mu-cosal margins should be taken. Next, take
the soft tissue margins. These can be taken as perpendicu-lar sections from the
anterior surface of the speci-men and from any other areas where the soft
tissues appear infiltrated by tumor.
Once all
the margins are taken, turn your atten-tion to the tumor. Keeping the three
anatomic regions of the larynx (the supraglottis, glottis, and subglottis) in
mind, carefully document the side, size, and exact location of any tumors. Also
note whether the tumor is endophytic or exophytic. Submit sections of each
identified tumor for histology to show its maximal depth of invasion as well as
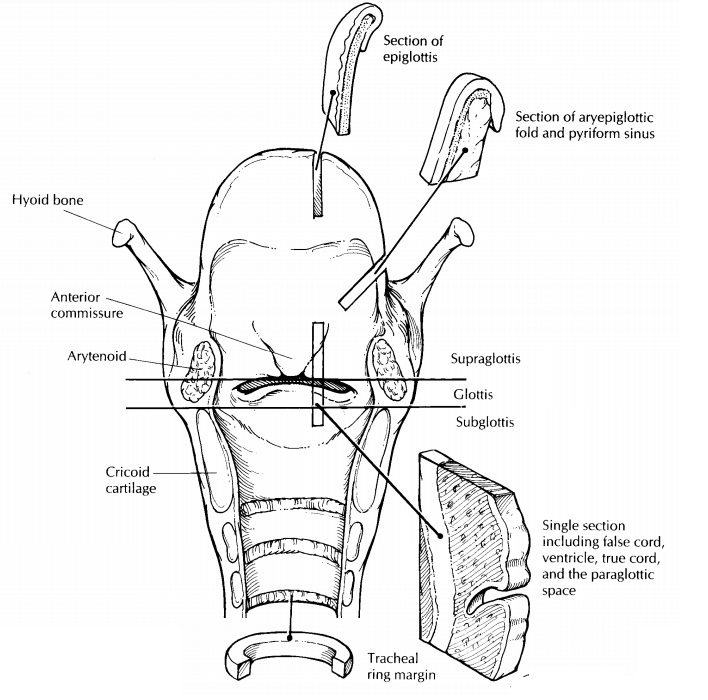
its relationship to grossly uninvolved mucosa. Next, carefully examine,
document, and sample for histology the mucosa of the pyriform sinuses, the
epiglottis, the aryepi-glottic folds, the false cords, the ventricles, the true
vocal cords, the anterior commissure, and the subglottis. In general,
longitudinal sections are most informative. As illustrated, a single
lon-gitudinal section can be taken to include the false cord, the ventricle, and
the true cord. Carefully examine the thyroid cartilage and the cricoid
cartilage. These structures should be selectively sampled to document the
presence or absence of tumor invasion. These sections may have to be submitted
for decalcification. If a tracheostomy site is present it should be noted, and
several sections of it should be submitted for histologic examination. Finally,
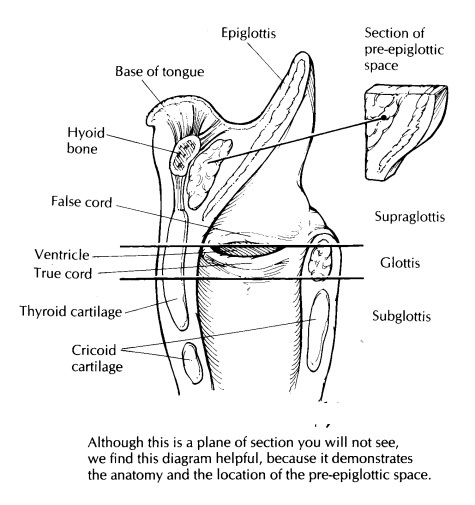
remember the three addi-tional anatomic landmarks discussed earlier. The
pre-epiglottic space can be sampled by taking a midline section from the base
of the epiglottis superiorly and anteriorly toward the hyoid bone. As
illustrated, the paraglottic space is usually in-cluded in the histologic
section of the true and false cords. Finally, a section of the anterior
com-missure should be submitted in cancers that in-volve the vocal cords.
If any organs were removed along with the larynx, their presence should be documented. Be especially diligent in your search for the thy-roid gland. Often, only a portion of the gland is removed with the larynx, and it may be embedded within the anterior soft tissues and strap muscles. If the thyroid gland is present, ex-amine it as described in the thyroid section and remember to look for para-thyroid glands. If a radical neck dissection is attached, it can be removed and examined sepa-rately as described in the section on radical neck dissections .
Related Topics