Chapter: Pathology: Male Pathology
Testicular Cancer
TESTICULAR CANCER
Testicular cancer typically presents with a
firm, painless testicular mass; nonsemi-nomatous tumors may present with
widespread metastasis. Caucasians have a higher incidence than African
Americans.
Risk factors include:
•
Cryptorchidism (3–5 times increased risk)
•
Testicular dysgenesis (testicular feminization and Klinefelter
syndrome)
•
Positive family history
Clinically, U/S typically
shows a hypoechoic intratesticular mass. Serum tumor marker studies can be
helpful in confirming the diagnosis. Treatment is radical orchiectomy and
possible chemotherapy/radiotherapy. Staging includes examination of the
surgically resected specimen, including a lymph node dissection, along with
imaging studies and lab tests.
Serum markers are used to
monitor disease.
•
AFP is produced by yolk sac tumors.
•
β-hCG is produced by choriocarcinoma and any tumor with
syncytiotropho-blastic giant cells.
•
LDH is used to measure tumor burden.
Germ Cell Tumors
Germ cell tumors are usually
hyperdiploid.
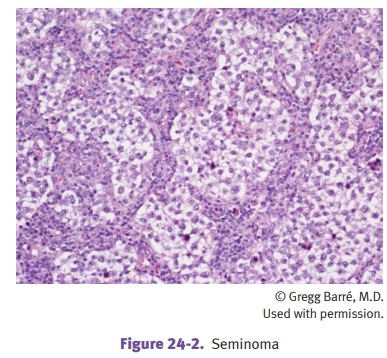
Seminoma is the most common germ cell tumor in adults, with mean age 40. It
is characteristically sensitive to both chemotherapy and radiation, and has an
excel-lent prognosis (early stage seminoma has 95% cure rate).
A variant is spermatocytic
seminoma, a disease of older men, also with an excellent prognosis.On gross
examination the tumor has a pale tan, bulging cut surface. Microscopic exam
shows sheets of monotonous cells (with clear cytoplasm and round nuclei)
separated by fibrous septae. Lymphocytes, granulomas, and giant cells may be
seen
Choriocarcinoma is a highly malignant tumor
that often has widespread metastasis at the time of diagnosis;
hematogenous spread to lungs and liver is particularly com-mon. The often small
tumor has extensive hemorrhage and necrosis. Microscopi-cally,
syncytiotrophoblasts and cytotrophoblasts are seen.
Yolk sac tumor (endodermal sinus tumor) is the most common germ cell
tumor in children; in pediatric cases, the prognosis is
good. In adults, the prognosis may depend on the other histologic types that
are admixed. Microscopically, yolk sac tumors show numerous patterns.
Schiller-Duval bodies are glomeruloid structures.
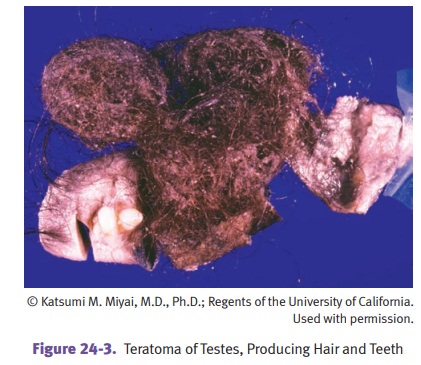
Teratoma often causes cystic masses which may contain
cartilage and bone. Micro-scopically, mature teratoma usually contains
ectodermal, endodermal, and meso-dermal tissue in a haphazard arrangement.
Immature elements contain embryonic tissue. Prepubertal cases are benign
regardless of immature elements; teratomas in adults have malignant potential.
Mixed germ cell tumors. As many as 60% of germ cell tumors contain >1
component. When both teratoma and embryonal carcinoma are present, the name
teratocarci-noma is used.
Sex Cord–Stromal Tumors
Sex cord–stromal tumors include Leydig cell and Sertoli cell tumors.
Leydig cell tumors cause
painless testicular masses, and have a bimodal distri-bution (prepubertal and
age >50). They may produce androgens and estrogens.
•
In adults, the hormonal secretion can produce gynecomastia; in
chil-dren, it can produce precocious puberty.
•
Benign tumors (90%) have an excellent prognosis; malignant tumors (10%)
can be refractory to chemotherapy and radiation therapy.
•
Tumor cells have abundant pink cytoplasm.
Sertoli cell tumors are rare and usually benign. Microscopically,
they show tubule formation.
Other Tumors
•
Testicular
lymphoma is the most common testicular tumor in men >age 60. It is most commonly non-Hodgkin lymphoma, diffuse
large cell type.
•
Scrotal
squamous cell carcinoma is associated with exposure to soot (chimney sweeps).