Chapter: Essentials of Psychiatry: Substance Abuse: Hallucinogen- and MDMA-Related Disorders
Substance Abuse: Hallucinogen- and MDMA-Related Disorders
Substance Abuse: Hallucinogen- and
MDMA-Related Disorders
Hallucinogens alter perception, cognition and mood
as their pri-mary psychobiological action in the presence of an otherwise clear
sensorium. LSD is the most common hallucinogen and is readily and cheaply
available in the USA. Unlike the chronic use of stimu-lants amphetamine and
cocaine, chronic use of hallucinogen does not lead to physiological dependence.
On the other hand tolerance to LSD builds in 4 to 7 days. There is no
withdrawal or documented fatalities from overdose of LSD. The
3,4-methylenedioxymeth-amphetamine (MDMA or Ecstasy) is a synthetic amphetamine
analogue that is used to enhance affiliative emotional responses. Its use
appears to be increasing, particularly among young adults. Dependence and
escalation of dosage are uncommon. All these agents are neurotoxic with
deleterious effects on serotonergic neurons, memory and mood. Common naturally
occurring com-pounds include mescaline (and peyote), psilocybin and
dimethyl-tryptamine (DMT). The dawn of modernity for synthetic halluci-nogenic
drugs can be placed tothe moment in 1943 when Albert Hofmann, a Swiss chemist,
discovered the potent psychological effects of LSD. The definition of an
hallucinogenic drug has been a matter of controversy. To address the problem of
classification, one may define as hallucinogenic “any agent which has
alterations in perception, cognition, or mood as its primary psychobiological
actions in the presence of an otherwise clear sensorium”.
Epidemiology of Hallucinogen Abuse
Among hallucinogens, LSD remains the most popular
in its class among American high school students. An annual drug survey of 45
000 students by the Monitoring the Future Program of the Uni-versity of Michigan
has been performed since 1975. There is a sta-ble long-term trend of LSD
lifetime use among one in 10 seniors.
Etiology and Pathophysiology
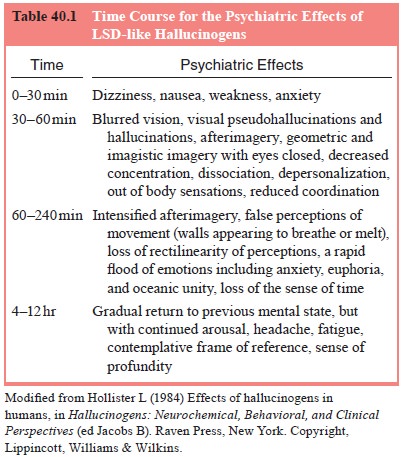
The acute effects of “tripping” on LSD-like (i.e,
with similar psychic effects, such as psilocybin or mescaline) hallucinogens
are variable and profound. Table 40.1 illustrates a typical time course for the
psychiatric effects of LSD.
The effective hallucinogenic doses vary widely
between drugs in this class, and between individuals. The conventional explanation
of this variability of response is instructional set, anticipation of drug
effects due to previous experience, and
environmental setting affect outcome. Additionally,
personal-ity, preexisting mental illness and genetic vulnerability are also
likely to be important. Unlike the chronic use of stimulants like amphetamine
and cocaine, chronic use of hallucinogens does not lead to physiological
dependence. On the other hand, tolerance to LSD rapidly builds in 4 to 7 days,
and lasts 3 days. Titeler and colleagues (1988) have shown that hallucinogenic
potency of LSD and selected phenylisopropylamines correlates with the drug’s
ability to bind at the postsynaptic 5-HT2 receptor.
Hallucinogens simultaneously decrease spontaneous
ac-tivity in the locus coeruleus, considered a novelty detector in the
midbrain, while enhancing sensory responses of the locus coeru-leus by
activating N-methyl-D-aspartate
receptors. In the cerebral cortex, the drugs both inhibit and induce activity
by exciting GABAergic and glutamatergic neurons respectively
The presence of selective serotonin reuptake
inhibitors blunts hallucinogenic effects, possibly through the activation of
5-HT1 receptors (Aghajanian and Marek, 1999). GABA-A
antianx-iety agents (e.g., benzodiazepines) promptly bring a bad trip to an
end, presumably by inhibition of the locus coeruleus. Opiates are likely to
have a similar outcome by reducing glutamatergic excitation of cortical
systems. This may explain why hallucinogen abuse appears to be so uncommon
among active opioid abusers.
Related Topics