Chapter: Surgical Pathology Dissection : Radical Neck Dissection
Radical Neck Dissection
Radical Neck Dissection
Neck
dissections for the en bloc removal of cervi-cal lymph nodes come in a variety
of shapes and sizes. The radical neck dissection is the stan-dard procedure to
which all other neck dissec-tions are compared. It includes resection of the
sternocleidomastoid muscle, the internal jugular vein, the spinal accessory
nerve, and the lymph nodes from levels I to V. The goal of the surgical
pathologist in evaluating these specimens is simply to identify the number of
lymph nodes involved by tumor at each level.
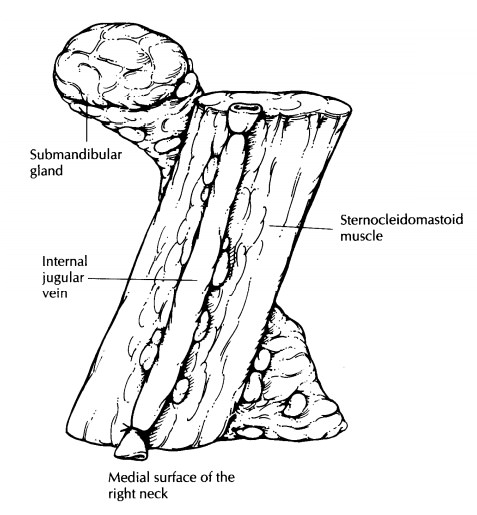
Start by
orienting the specimen. The dissection is shaped like a Z. The pink-tan,
lobulated sub-mandibular gland is usually easy to identify, and it occupies
level I, the most anterosuperior aspect of the specimen. The internal jugular
vein, as its name implies, is present on the internal (medial) surface of the
sternocleidomastoid muscle. Using these two anatomic landmarks, one can both
orient the specimen and determine which side it was taken from. After orienting
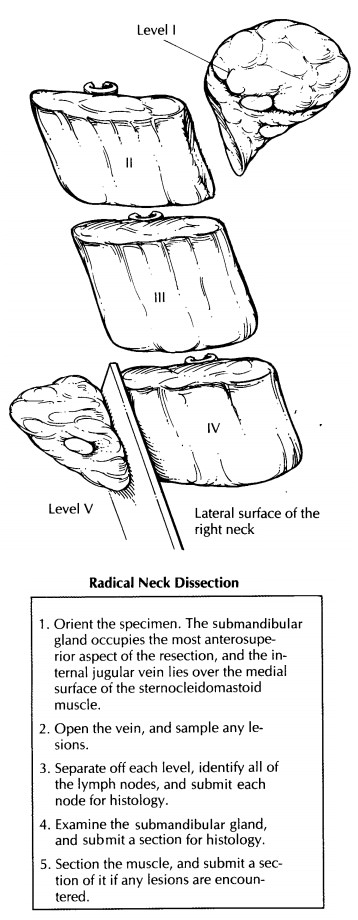
the specimen, measure its overall dimensions. Next, open the jugular vein along
its length, and look for tu-mor involvement or thrombosis. Sample any
abnormality in the vein.
The
specimen can now be divided into its five levels and each level separately
dissected for lymph nodes. First, dissect off level I, which in-cludes the
submandibular salivary gland and the triangle of soft tissues anterior to the
sternoclei-domastoid muscle. Next, remove level V, the triangle of fatty
connective tissue posterior to the muscle. Finally, levels II, III, and IV can
be separated off by dividing the sternocleidomas-toid muscle into equal thirds.
Level II, the upper jugular group, is composed of the lymph nodes around the
upper third of the sternocleidomas-toid muscle. Level III, the middle jugular
group, is composed of the lymph nodes around the middle third of the
sternocleidomastoid mus-cle, and level IV, the lower jugular group, is composed
of lymph nodes around the lower third. Now search for the lymph nodes. The best
place to look for lymph nodes in each level is in the fatty connective tissue.
Lymph nodes usually will not be found within the sternoclei-domastoid muscle
itself. Section each lymph node at 2- to 3-mm intervals along its long axis. If
the lymph node is grossly uninvolved by tumor, submit the entire lymph node for
histo-logic examination. If the lymph node is grossly involved by tumor,
measure the size of the im-plant and submit two sections of the metastasis. Be
sure that these two representative sections include the lymph node capsule
along with a rim of the perinodal fat so you will be able to determine the
presence or absence of extranodal tumor spread. In addition, the salivary gland
in level I should be measured, described, and serially sectioned. If any masses
are found in the salivary gland, If no abnor-malities are grossly apparent,
simply submit a representative section for histology. Finally, representative
sections of any tumor involving the sternocleidomastoid muscle or extranodal
soft tissue should be submitted for histology. If a group of matted lymph nodes
is present, it will be impossible to dissect out each individual lymph node. In
these cases, submit two sections through each level involved to document the
extensive nature of the tumor.
A number
of variations of the neck dissection exist. These are well described by Robbins
and co-workers.2 In a modified neck
dissection, for example, lymph nodes from levels I through V are removed,
but one or more of the three major structures (internal jugular vein, spinal
accessory nerve, sternocleidomastoid muscle) is not in-cluded in the
dissection. Selective neck dissections
differ from radical and modified neck dissec-tions in that lymph nodes from
only some of the five levels are removed. Each of these can be dissected using
the same approach outlined above. First, orient the specimen. Without
im-portant land marks (e.g., submandibular gland, internal jugular vein), you
will usually have to rely on the surgeon to designate each level. Second,
identify the lymph nodes at each level. Third, submit each node for histology.
Important Issues to Address in Your Surgical Pathology Report on Radical Neck Dissections
· What procedure was performed, and what structures/organs are present?
·
What is the total number of lymph nodes
pres-ent at each level, and how many of these are involved by tumor?
·
What is the size of the largest metastasis?
·
Does the carcinoma extend beyond the lymph node
and into extranodal soft tissue?
·
Is the internal jugular vein thrombosed and/ or
infiltrated by tumor?
·
Do the salivary glands, muscle, and soft
tissues contain tumor or any other pathology?
Related Topics