Chapter: Ophthalmology: Pupil
Pupil: Examination Methods
Examination Methods
Complete examination of the pupilincludes
testing direct and indirect light reflexes, the swinging flashlight test,
testing the near reflex, and morphologic evaluation of the iris. A synopsis of
all findings is required to determine whether a disorder is due to ocular or
cerebral causes .
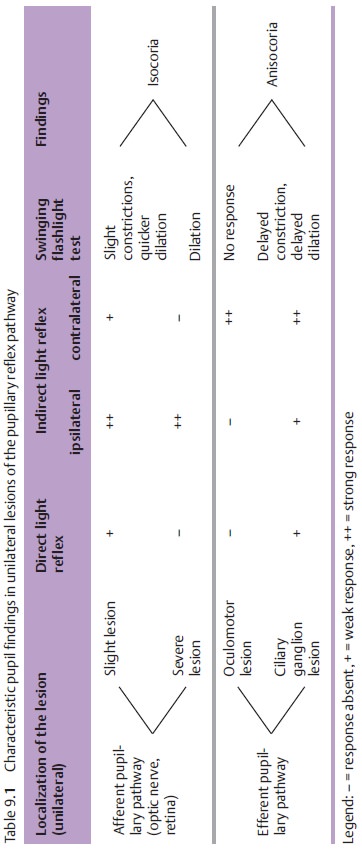
Testing the Light Reflex (Table 9.1)
Light reflex is tested in subdued daylight
where the pupil is slightly dilated.
The patient gazes into the distance to
neutralize near-field miosis.
Direct light reflex:
The examiner first covers both of the patient’s eyes,
thenuncovers one eye. Normally the pupil will constrict after a latency period
of about 0.2 seconds. The other eye is tested in the same manner.
Indirect or consensual light reflex:
The examiner separates the patient’seyes by placing his or her hand on the bridge of the patient’s nose. This pre-vents incident light from directly striking the eye being examined, which would elicit a direct light reflex. The examiner then illuminates the other eye while observing the reaction of the covered, non-illuminated eye. Normallyboth pupils will constrict, even in the non-illuminated eye.
Swinging flashlight test:
This test is used to diagnose adiscrete unilateral orunilaterally more pronounced sensory deficit in
the eye (optic nerve and/or ret-ina). Often damage to the optic nerve or retina
is only partial, such as in partial atrophy of the optic nerve, maculopathy, or
peripheral retinal detachment. In these cases, the remaining healthy portions
of the afferent pathway are suffi-cient to trigger constriction of the pupil
during testing of the direct light reflex. This constriction will be less than
in the healthy eye but may be diffi-cult to diagnose from discrete pupillary
reflex findings alone. Therefore, the reflexive
behavior of both eyes should be evaluated in a direct comparison todetect
differences in the rapidity of constriction and subsequent dilation. This is
done by moving a light source alternately from one eye to the other in what is
known as a swinging flashlight test.
Reproducible results can only obtained if the
examiner strictly adheres to this test protocol:
❖The patient focuses on a remote object in a
room with subdued light. This neutralizes convergence miosis, and the pupils
are slightly dilated, making the pupillary reflex more easily discernible.
❖The examiner alternately illuminates both eyes
with a relatively bright light, taking care to maintain a constant distance, duration of illumination,and light intensity so
that both eyes must adapt to the same conditions.
❖The examiner evaluates the initial constriction upon illumination and the subsequent dilation of the pupil.
Where the pupil constricts more slowly and
dilates more rapidly than in the fellow eye, one refers to a relative afferent pupillary defect. The
defect is “rela-tive” because the difference in pupillary reflex only occurs
when there is a difference in the sensory defect to the left and right eyes.
Evaluating the Near Reflex
The near reflex triad consists of:
1. Convergence of the visual axes.
2. Accommodation.
3. Constriction of the pupils (miosis).
The near reflex is tested by having the patient focus on a distant object and then on an object in the near field. Usually this is the patient’s finger, which is brought to within 10 cm of the eyes. The near reflex is intact if both eyes con-tinuously converge with accommodation and miosis appropriate for the patient’s age as the object is moved to within 10 cm of the eyes. The examiner should take care to avoid illuminating the pupil, which will produce a light reflex with miosis.
Related Topics