Chapter: Maternal and Child Health Nursing : Puerperium
Psychology of puerperium
Psychology of puerperium
Most
women are happy during Puerperium. Some may be anxious, apprehensive and
sensitive. These groups of women cry easily and find the task of caring for the
baby too cumbersome. The midwife needs to be understanding in her dealings with
the mother. Mothers are always appreciative of the midwife’s advice, kind
approach, assurance, and assistance.
Puerperium
is a period of excitement, the mother is eager to share her experiences with
partner, family and friends.
Physiology of puerperium
These are
the changes that take place after delivery. This is characterized by endocrine
activity. Oxytocin acts upon the uterine muscle and breast tissue. In the 3rd
stage the action brings about the separation of the placenta and prevents
hemorrhage (by the action of living ligature) and initiation of lactation.
Other changes include the lochia which undergo sequential changes as involution
progresses. The main changes occur in the uterine and decidua but the ligament
also return to their former state prior to pregnancy. The stretched vagina,
pelvic floor and perineum regain their tone but, in some instances a degree of laxity
persists. There is a dramatic reduction in the level of estrogen and
progesterone reaches basal level by the 7th day if she breastfeeds,
otherwise the oestradiol begins to rise 14 – 21 days after birth indicating a
resumption of ovarian follicle development and later ovulation
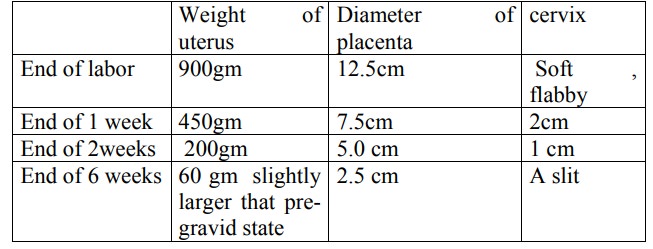
Involution of the uterus:
Return of the uterus to its
pre-gravid state. The reduction in the size of the uterus is brought about by
the process known as Autolysis and Ischaemia i.e. self digestion of the uterine
muscle fibres by proteolytic enzymes and self destruction. The end results are
removed by the phagocytic action of polymorphs and macrophages in the blood and
lymphatic system which invades the collagen fibres between the myometrial cells
and remove the fat from the area. This process is further assisted by the
contraction and retraction of the uterine muscles under the influence of
oxytocin resulting in the compression of blood vessels and reducing uterine
blood flow causing the release of more lochia and after pain during breast
feeding. Involution reduces the size of the uterus by about 1.6 in. (about a
finger breath) a day.
Progressive
changes in the uterus after delivery
The
remains of the spongy layer of the decidua are shed. At the end of the 8th
week, the placenta site is healed and a new endometrium is regenerated. After
about 4 or more weeks menstruation may commence, by the 12th day of
Puerperium the uterus has shrunk behind the symphysis pubis.
Lochia
This is
the term given to the discharges from the uterus during the Puerperium. They
are alkaline in reaction and organism flourish more in it than in the acid
vaginal secretion. The amount varies in
women and
more in quantity than menstrual flow. The odor is heavy and unpleasant but not
offensive, similar to menstrual flow. Lochia undergo changes as involution
progresses. The volume is described as heavy, moderate and scanty
Progressive changes
·
Lochia rubra (red): 1 – 4 days of Puerperium. For t
he first 3 days the lochia consist mainly of blood, shred of decidua and
fragments of chorion, amniotic fluid, laguno vernix caseosa and meconium.
·
Lochia serosa (pink): 5 – 9 days. The discharge is
paler and brownish in color. It contains less blood and more serum. Also contains
leucocytes and organism , no clots
·
Lochia Alba (white) 10 –15 days: the discharge is c
reamy greenish in color and contains leucocytes, organisms, cervical mucus and
debris from healing process in the uterus and vagina. Slight blood
discoloration may be seen for a further 2—3 weeks. A persistent red lochia is a
warning s ign of retained product of conception and likelihood of puerperal
hemorrhage and this should be reported without delay.
Urinary system
Kidneys: renal action is increased in
early part of Puerperiummore urine is passed because of reduction of blood
volume (red cell mass) from its raised pregnancy levels and excretion of waste
products of autolysis.
Bladder in the first few days micturation
may be difficult partlybecause of reflex suppression of the destrusor activity
and sphincters spasm from irritation of the levator ani muscle during delivery
or odema of the urethra. During the first 1 or 2 days marked diuresis occurs
due to falling progestrone and alteration of cell metabolism to the
non-pregnant state.
Circulatory System:
During pregnancy circulatory
volumeincreases by 50%,this places exact strain on the heart. The cardiac
output immediately after delivery increases for about 48 hrs returing to
pre-gravid level in 4 weeks. Fluid loss result from diaphoresis (profuse
perspiration) and diuresis (urinary output) during labor and childbirth is
approximately 2.2kg. Up to 500mls of blood may be lost in normal delivery.
Amniotic fluid is another source during birth. The cardiovascular system has to
quickly adjust itself to these changes. It also results in improvement in
varicosities. There is relief of pressure on the vena cava placed on it by the
gravid uterus.
Blood
changes : in the last 4 weeks of pregnancy there is a significant rise in the
levels of fibrous plasmogen factors II,VII,VIII &X. A few days a rapid fall
in fibrogen plasminogen factor VIII level occurs while there is a rise in
circulating fibrinogen degradation products, probably due to the lysis of
fibrin deposits in placenta bed. By the 2nd week of Puerperium the
coagulability of the blood is altered and increases risk of thrombosis is
present. The normal non-pregnant red cell levels are reached about the 40th
day.
Musculo-Skeletal System:
The
stretching muscles and lossof tone of abdominal muscles during pregnancy
results in flabby appearances of the abdomen immediately after delivery. This
normally responds to exercise and involution and gradual tightening of pelvic
muscles and ligaments. This is however faster and better with primiparae than
multiparae.
Nervous systems: this is normally unaffected
except for theeffects of drugs during labor
Integumentary: striae gravidarum become lighter
and silvery;gradual disappearance of linea nigra, chloasma gravidarum and
nipple hyperpigmentation. With exercise and good diet circulation, muscle tone,
skin elasticity and healing improves.
Respiratory:after
child birth many women are able to breatheeasily. Shortness of breath at
anytime after child birth requires further assessment to rule out underlying
pathophiology ; Post – Partum Hemorrhage (PPH) .
Gastrointestinal system:some
women experience constipation inpuerperium which may be attributed to
relaxation of abdominal wall and loss of intra-abdominal pressure. The presence
of hemorrhoids or an episiotomy may cause some discomfort during bowel
movement.
Breasts: the female breast undergoes
changes during pregnancy inpreparation for lactation and breast feeding.
Colostrums supply the neonate with good nourishment. It contains more protein
and salts (NaCl, Zinc) but less fat & Carbohydrate. The breast milk is
secreted in the last month to 3 days postpartum when breast milk appears. It is
rich in antibodies, acts as laxative aiding massage of mechonium. Lactation
begins 48-72hrs after child birth, but not fully established until about 10
days after birth.
Related Topics