Chapter: Obstetrics and Gynecology: Premature Rupture of Membranes
Premature Rupture of Membranes: Diagnosis
DIAGNOSIS
Fluid
passing through the vagina must be presumed to be amniotic fluid until proved
otherwise.
At times, patients describe a
“gush” of fluid, whereas at other times they note a history of steady leakage
of small amounts of fluid. Intermittent urinary leakage is common during
pregnancy, especially near term, and this can be confused with PROM. Likewise,
the normally increased vaginal secretions in pregnancy as well as perineal
moisture (espe-cially in hot weather) may be mistaken for amniotic fluid.
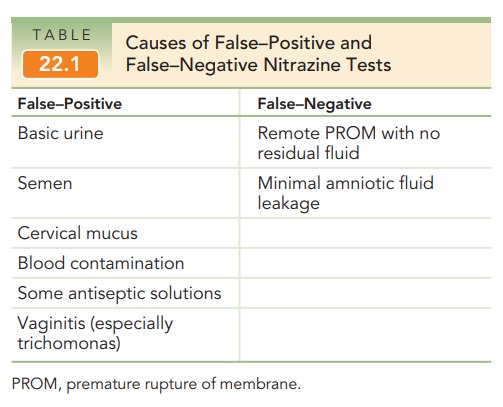
The nitrazine test uses pH to distinguish amniotic fluid from urine and
vaginal secretions. Amniotic fluid is alkaline, having a pH above 7.1; vaginal
secretions have a pH of 4.5 to 6.0, and urine has a pH of ≤6.0. To perform the nitrazine
test, a sample of fluid obtained from the vagina during a speculum examination
is placed on a strip of nitrazine paper. If the pH is 7.1 to 7.3, reflecting
that of amniotic fluid, the paper turns dark blue. Cervical mucus, blood, and
semen are possible causes of false-positive results (Table 22.1).
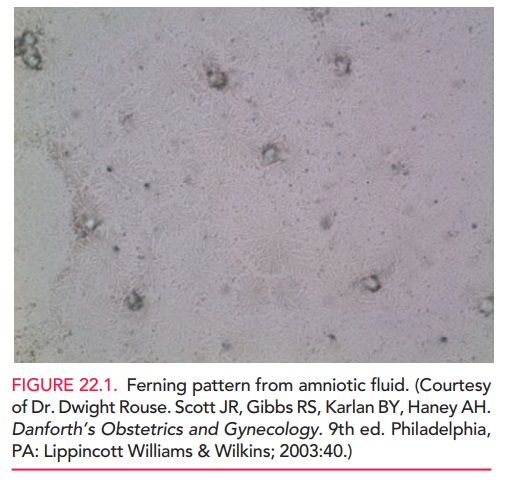
The fern test is also used to distinguish amniotic fluid from other fluids. It is named for the pattern of arboriza-tion that occurs when amniotic fluid is placed on a slide and is allowed to dry in room air. The resultant pattern, which resembles the leaves of a fern plant, is caused by the sodium chloride content of the amniotic fluid. The ferning pattern from amniotic fluid is fine, with multiple branches, as shown in Figure 22.1; cervical mucus does not fern or, if it does, the pattern is thick with much less branching. This test is considered more indicative of ruptured membranes than the nitrazine test, but as with any test it is not 100% reliable.
Ultrasonography can be helpful in
evaluating the possi-bility of rupture of membranes. If ample amniotic fluid
around the fetus is visible on ultrasound examination, the diagnosis of PROM
must be questioned. However, if the amount of amniotic fluid leakage is small,
sufficient amni-otic fluid will still be visible on scan. When there is less
than the expected amount of fluid seen on ultrasound, the differ-ential
diagnosis of oligohydramnios, including PROM must be considered. When the clinical history or
physicalexamination is unclear, membrane rupture can be diagnosed unequivocally
with ultrasonographically guided transabdomi-nal instillation of indigo carmine
dye, followed by observation for passage of blue fluid from the vagina. This
procedure isperformed very infrequently, however.
The differential diagnoses for PROM include urinary incontinence,
increased vaginal secretions in pregnancy (physiologic), increased cervical
discharge (pathologic, e.g., infection), exogenous fluids (such as semen or
douche), and vesicovaginal fistula.
Related Topics