Chapter: Pathology: Pancreatic Pathology
Pancreatic Tumors
PANCREATIC TUMORS
Pancreatic neuroendocrine tumors (islet cell tumors) are less
common than exocrine tumors. Most are considered low grade malignancies. Some
patients lack laboratory evidence of hormone overproduction. These tumors are
not distinguishable from each other on the basis of gross appearance or
histology.
•
Insulinoma (β-cell tumor) (most common type of islet cell
tumor)
o
Produces insulin
o
Can cause hypoglycemia,
sweating, hunger, confusion, and insulin coma
o
Surgical excision is
curative
•
Gastrinoma (G-cell tumor)
o
Produces gastrin
o
Excess gastrin manifests
as Zollinger-Ellison syndrome, which is charac-terized by thick gastric folds,
elevated serum gastrin, gastric hyperacid-ity, and intractable peptic ulcers
o
Gastrinomas may arise
outside the pancreas
o
May be associated with MEN
I
•
Glucagonoma (α-cell tumor)
o
Produces glucagon
o
Excess glucagon causes
hyperglycemia (diabetes), anemia, and skin rash
•
Somatostatinoma (δ-cell tumor)
•
Produces somatostatin
•
Excess somatostatin
inhibits insulin secretion, leading to diabetes
•
Can also inhibit gastrin
secretion (leading to hypochlorhydria) and cho-lecystokinin secretion (leading
to gallstones and steatorrhea)
•
Prognosis is poor
•
VIPoma
o Produces vasoactive
intestinal peptide (VIP)
o Excess VIP causes
WDHA syndrome: watery diarrhea, hypokalemia, and achlorhydria
Pancreatic
carcinoma is the fifth most
common cause of cancer death in the United
States,
and the incidence is rising.
•
Most common ages 60-80
•
Smoking is a risk factor
•
Presents with only vague signs and symptoms until late in
course
•
When more definitive signs and symptoms develop, they can
include abdomi-nal pain, migratory thrombophlebitis, and obstructive jaundice
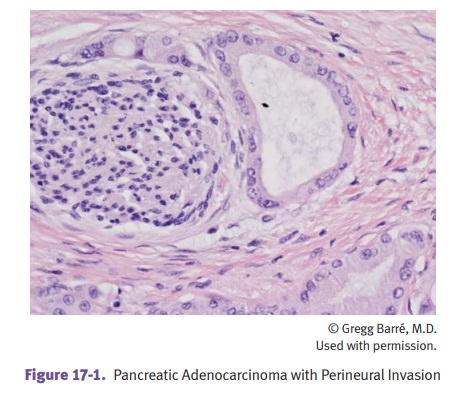
The tumor may occur in the head
(60%), body (15%), and tail (5%). Microscopi-cally, the adenocarcinoma arises
from the duct epithelium. Tumor desmoplasia and perineural invasion are common.
Tumor markers for pancreatic carcinoma include CEA and CA19-9, but they are not
useful screening assays.
Treatment is
surgical excision (Whipple procedure). The prognosis is very poor, with 5-year
survival only ~5%.
Pancreatic cystic neoplasms: Serous neoplasms account for 25%
of pancreatic cystic neoplasms; most are
benign (cystadenomas) and the tumors carry a mutation of VHL.
Mucinous neoplasms: Mucinous cystic
neoplasms are common in women and can
harbor
dysplasia or carcinoma; distal pancreatectomy is curative in most cases. Intraductal papillary mucinous neoplasms are common in men
and tend to arise in the head of the
pancreas; GNAS mutations are common
and carcinoma may arise in the neoplasm.