Chapter: Essentials of Psychiatry: Diagnostic Classification in Infancy and Early Childhood
Overview of the Classification System - Infancy and Early Childhood
Overview of the Classification
System
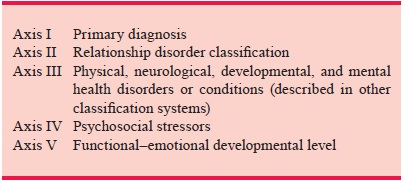
DC:0–3 proposes a provisional multiaxial
classification system. We refer to the classification system as provisional
because it is assumed that categories may change as more knowledge
accumu-lates. The diagnostic framework consists of the following
The axes in this system are not intended to be
entirely symmetrical with such other systems as DSM-IV and the In-ternational Statistical Classifi cation
of Diseases and Related Health Problems, 10th Revision (ICD-10) because
this system, in dealing with infants
and young children, focuses on devel-opmental issues. Dynamic processes, such
as relationship and developmentally based conceptualizations of adaptive
patterns (i.e., functional–emotional developmental level), are therefore of
central importance.
Use of the system will provide the psychiatrist
with a “di-agnostic profile” of an infant or toddler. Such a diagnostic
pro-file focuses the psychiatrist’s attention on the various factors that are
contributing to the infant’s difficulties as well as on areas in which
intervention may be needed.
Axis I: Primary Diagnoses
The following are the Axis I primary diagnoses that
have thus far been suggested:
100.
Traumatic Stress Disorder
A continuum of symptoms related to a single event,
a series of connected traumatic events, or chronic enduring stress.
a)
Reexperiencing of the trauma, as evidenced by
i)
post traumatic play
ii) recurrent
recollections of the traumatic event outside play
iii) repeated
nightmares
iv) distress
at reminders of the trauma
v) flashbacks
or dissociation
b) Numbing
of responsiveness or interference with develop-mental momentum
i)
increased social withdrawal
ii) restricted
range of affect
iii) temporary
loss of previously acquired developmental skills
iv) a
decrease in play
c)
Symptoms of increased arousal
i)
night terrors
ii) difficulty
going to sleep
iii) repeated
night waking
iv) significant
attentional difficulties
v) hypervigilance
vi) exaggerated
startle response
d) Symptoms
not present before
i)
aggression toward peers, adults, or animals
ii) separation
anxiety
iii) fear of toileting
alone
iv) fear of
the dark
v) other new
fears
vi) self-defeating
behavior or masochistic provocativeness
vii) sexual
and aggressive behaviors
viii)
other nonverbal reactions (e.g., somatic symptoms,
mo-tor reenactment, skin stigmas, pain, or posturing)
200.
Disorders of Affect
Focuses on the infant’s experience and on symptoms
that are a general feature of the child’s functioning rather than specific to a
situation or relationship.
201. Anxiety Disorders of Infancy and Early
Childhood
Levels of anxiety or fear, beyond expectable
reactions to normal developmental challenges.
e)
Multiple or specific fears
i)
Excessive separation or stranger anxiety
ii) Excessive
anxiety or panic without clear precipitant
iii) Excessive
inhibition or constriction of behavior
iv) Lack of development
of basic ego functions
v) Agitation,
uncontrollable crying or screaming, sleeping and eating disturbances,
recklessness, and other behaviors Criterion: Should persist for at least 2
weeks and interfere with appropriate functioning.
202. Mood Disorder: Prolonged Bereavement–Grief
Reaction
vi) Possible
crying, calling and searching for the absent par-ent, refusing comfort
vii) Emotional
withdrawal, with lethargy, sad facial expres-sion, and lack of interest in
age-appropriate activities
viii)
Eating and sleeping possibly disrupted
ix) Regression
in developmental milestones
x) Constricted
affective range
xi) Detachment
xii) Sensitivity
to any reminder of the caregiver
203.Mood Disorder: Depression of Infancy and Early
Childhood
Pattern of depressed or irritable mood with diminished
interest or pleasure in developmentally appropriate activities, diminished
capacity to protest, excessive whining, and diminished social interactions and
initiative. Disturbances in sleep or eating. Criterion: At least 2 weeks.
204. Mixed Disorder of Emotional Expressiveness
Ongoing difficulty expressing developmentally
appropriate emotions.
i)
The absence or near-absence of one or more specific
types of affects
ii) Constricted
range of emotional expression
iii) Disturbed
intensity
iv) Reversal
of affect or inappropriate affect
205. Childhood Gender Identity Disorder
2.
Becomes manifest during the sensitive period of
gender identity development (between approximately 2 and 4 years).
i)
A strong and persistent cross-sex identification
ii) repeatedly
states desire to be, or insistence that he or she is, the opposite sex
iii) in boys,
preference for cross-dressing or simulating fe-male attire; in girls,
insistence on wearing stereotypical masculine clothing
iv) strong
and persistent preferences for cross-sex roles in fan-tasy play or persistent
fantasies of being the opposite sex
v) intense
desire to participate in the games and pastimes of the opposite sex
vi) strong
preference for playmates of the opposite sex
b) Persistent
discomfort with one’s assigned sex or sense of inappropriateness in that role
c)
Absence of nonpsychiatric medical condition
206. Reactive Attachment Deprivation–Maltreatment
Disorder of Infancy
i)
Persistent parental neglect or abuse, of a physical
or psy-chological nature, undermines the child’s basic sense of security and
attachment.
ii) Frequent
changes in, or the inconsistent availability of, the primary caregiver.
iii) Other
environmental compromises that prevent stable attachments.
300. Adjustment Disorder
3.
Mild, transient situational disturbances related to
a clear environmental event and lasting no longer than 4 months.
400. Regulatory Disorders
Difficulties in regulating physiological, sensory,
attentional, motor, or affective processes and in organizing a calm, alert, or
affectively positive state. Observe at least one sensory, sensory–motor, or
processing difficulty from the following list, in addition to behavioral
symptoms.
i)
Overreactivity or underreactivity to loud or high-
or low-pitched noises
ii) Overreactivity
or underreactivity to bright lights or new and striking visual images
iii) Tactile
defensiveness or oral hypersensitivity
iv) Oral–motor
difficulties or incoordination influenced by poor muscle tone and oral-tactile
hypersensitivity
v) Underreactivity
to touch or pain
vi) Gravitational
insecurity
vii) Underreactivity
or overreactivity to odors
viii)
Underreactivity or overreactivity to temperature
ix) Poor
muscle tone and muscle stability
x) Qualitative
deficits in motor planning skills
xi) Qualitative
deficits in ability to modulate motor activity
xii) Qualitative
deficits in fine motor skills
xiii)
Qualitative deficits in auditory–verbal processing
xiv)
Qualitative deficits in articulation capacities
xv) Qualitative
deficits in visual–spatial processing capacities
xvi)
Qualitative deficits in capacity to attend and
focus
401. Type I: Hypersensitive
b) Fearful
and cautious
i)
Behavioral patterns: excessive cautiousness,
inhibition, or fearfulness
ii) Motor and
sensory patterns: overreactivity to touch, loud noises, or bright lights
c)
Negative and defiant
i)
Behavioral patterns: negativistic, stubborn,
controlling and defiant; difficulty in making transitions; prefers repetition
to change
ii) Motor and
sensory patterns: overreactivity to touch and sound; intact visual–spatial
capacities; compromised auditory processing capacity; good muscle tone and
motor planning ability; shows some delay in fine motor coordination
402. Type II: Underreactive
d) Withdrawn
and difficult to engage
i)
Behavioral patterns: seeming disinterest in
relation-ships; limited exploratory activity or flexibility in play; appears
apathetic, easily exhausted and withdrawn
ii) Motor and
sensory patterns: underreactivity to sounds and movement in space; either
overreactive or underre-active to touch; intact visual–spatial processing
capaci-ties, but auditory–verbal processing difficulties; poor motor quality
and motor planning
e)
Self-absorbed
i)
Behavioral patterns: creative and imaginative, with
a ten-dency to tune into her or his own sensations, thoughts, and emotions
ii) Motor and
sensory patterns: decreased auditory–verbal processing capacities
403. Type III: Motorically Disorganized, Impulsive
Mixed sensory reactivity and motor processing difficulties. Some appear more
aggressive, fearless and destructive; others appear more impulsive and fearful.
i)
Behavioral patterns: high activity, seeking contact
and stimulation through deep pressure; appears to lack caution
ii) Motor and
sensory patterns: sensory underreactivity and motor discharge
404. Type IV: Other
500. Sleep Behavior Disorder
Only presenting problem; younger than 3 years of age; no accompanying
sensory reactivity or sensory processing difficulties. Difficulty in initiating
or maintaining sleep; may also have problems in calming themselves and dealing
with transitions from one stage of arousal to another.
600. Eating Behavior Disorder
Shows difficulties in establishing regular feeding
patterns with adequate or appropriate food intake. Absence of general
regulatory difficulties or interpersonal precipitants (e.g., separation,
negativism, trauma).
700. Disorders of Relating and Communicating
i)
DSM-IV conceptualization pervasive developmental
dis-order, or
ii) Multisystem
developmental disorder
·
Multisystem Developmental Disorder
i)
Significant impairment in, but not complete lack
of, the ability to form and maintain an emotional and social rela-tionship with
primary caregiver
ii) Significant
impairment in forming, maintaining, or devel-oping communication
iii) Significant
dysfunction in auditory processing
iv) Significant
dysfunction in the processing of other sensa-tions and in motor planning
701. Pattern A
These children are aimless and unrelated most of
the time, with severe difficulty in motor planning, so that even simple
intentional gestures are difficult.
702. Pattern B
These children are intermittently related and
capable, some of the time, of simple intentional gestures.
703. Pattern C
These children evidence a more consistent sense of
relatedness, even when they are avoidantor rigid
Axis II: Relationship Disorder Classification
The diagnostic system also includes an Axis II for
relationships classification. Three aspects of a relationship are considered:
1) behavioral quality of the interaction, 2) affective tone, and 3)
psy-chological involvement. The types of relationship problems are as follows:
901. Overinvolved Relationship
Physical or psychological overinvolvement.
i.
Parent interferes with infant’s goals and desires
ii.
Overcontrols
iii.
Makes developmentally inappropriate demands
iv.
Infant appears diffuse, unfocused and
undifferentiated
v.
Displays submissive, overly compliant behaviors
vi.
May lack motor skills or language expressiveness
902. Underinvolved Relationship
Sporadic or infrequent genuine involvement.
i.
Parent insensitive or unresponsive
ii.
Lack of consistency between expressed attitudes
about in-fant and quality of actual interactions
iii.
Ignores, rejects, or fails to comfort
iv.
Does not reflect infant’s internal feeling states
v.
Does not adequately protect
vi.
Interactions underregulated
vii.
Parent and infant appear to be disengaged
viii.
Infant appears physically or psychologically
uncared for
ix.
Delayed or precocious in motor and language skills
903. Anxious–Tense Relationship
Tense, constricted with little sense of relaxed
enjoyment or mutuality.
i.
Parent is overprotective and oversensitive
ii.
Awkward or tense handling
iii.
Some verbally and emotionally negative interactions
iv.
Poor temperamental fit between parent and child
v.
Infant compliant or anxious
904. Angry–Hostile Relationship
Harsh and abrupt, often lacking in emotional
reciprocity.
i.
Parent insensitive to infant’s cues
ii.
Handling is abrupt
iii.
Infant frightened, anxious, inhibited, impulsive,
or dif-fusely aggressive
iv.
Defiant or resistant behavior
v.
Demanding or aggressive behaviors
vi.
Fearful, vigilant and avoidant behaviors
vii.
Tendency toward concrete behavior
905. Mixed Relationship
Combination of the features described above.
906. Abusive Relationships
a)
Verbally abusive relationship.
i)
Intended to severely belittle, blame, attack,
overcontrol and reject the infant or toddler
ii) Reactions
vary from constriction and vigilance to se-vere acting-out behaviors
b) Physically
abusive relationship.
i)
Physically harms by slapping, spanking, hitting,
pinch-ing, biting, kicking, physical restraint, isolation
ii) Denies
food, medical care, or opportunity to rest
iii) May
include verbal and emotional abuse or sexual abuse
c)
Sexually abusive relationship.
i)
Parent engages in sexually seductive and
overstimulat-ing behavior – coercing or forcing child to touch par-ent
sexually, accept sexual touching, or observe others’ sexual behaviors
ii) Young
child may evidence sexually driven behaviors such as exhibiting himself or
herself or trying to look at or touch other children
iii) May
include verbal and emotional abuse or physical abuse
Axis III: Medical and Developmental Diagnoses
On Axis III, one indicates any coexisting physical (including
medical and neurological), mental health, or developmental dis-orders. DSM-IV,
ICD-9 or ICD-10 for the primary care setting classifications are used.
Occupational therapy, physical therapy, special education and other
designations are specified.
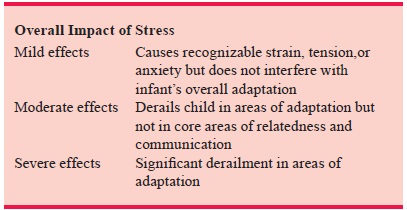
Axis IV: Psychosocial Stressors
On Axis IV, one identifies (1) the source of stress
(e.g., abduction, adoption, loss of parent, natural disaster, parent’s
illness), (2) se-verity (mild to catastrophic), (3) duration (acute to
enduring), and (4) overall impact (none, mild, moderate, severe)
Axis V: Functional–Emotional Developmental Level
Axis V profiles the child’s functional and
emotional developmen-tal level. It involves the following.
A. Essential processes or capacities
1.
Mutual attention: ability of dyad to attend to one
another
2.
Mutual engagement: joint emotional involvement
3.
Interactive intentionality and reciprocity: ability
for cause-and-effect interaction; infant signals and re-sponds purposefully
4.
Representational–affective communication: language
and play communicate emotional themes
5.
Representational elaboration: pretend play and
sym-bolic communication that go beyond basic needs and deal with more complex
intentions, wishes, or feelings
6.
Representational differentiation I: pretend play
and symbolic communication in which ideas are logically related; knows what is
real and unreal
7.
Representational differentiation II: complex
pretend play; three or more ideas are logically connected and informed by
concepts of causality, time and space
B. Functional–Emotional Developmental Level
Summary, which documents the child’s achievement
1.
Has fully reached expected levels
2.
At expected level but with constrictions – not full
range of affect; not at this level under stress; only with certain caregivers
or with exceptional support
3.
Not at expected level but has achieved all prior
levels
4.
Not at current expected level but some prior levels
5.
Has not mastered any prior levels
Related Topics